

For many living with Borderline Personality Disorder (BPD), the most daunting symptom isn’t the emotional volatility or the fractured relationships—We see the pervasive sense that things will never get better. This feeling of permanence often stems from a legacy of clinical pessimism, where BPD was once viewed as a lifelong sentence of instability. But, modern psychiatric data tells a radically different story, suggesting that recovery from Borderline Personality Disorder is not only possible but statistically probable for a majority of patients.
The journey toward stability is rarely linear. It often begins with a period of acute crisis, characterized by intense emotional dysregulation and a struggle to maintain a consistent sense of self. For a 26-year-old facing these hurdles, the prospect of a “normal” life can feel like a mirage. Yet, longitudinal research indicates that BPD has one of the highest remission rates among all personality disorders, provided the individual has access to evidence-based care.
The shift in understanding comes from a move away from the idea of a “cure”—which implies the total erasure of a personality trait—toward the concept of “remission.” In clinical terms, remission occurs when a person no longer meets the full diagnostic criteria for the disorder. For many, In other words the “peaks and valleys” of their emotions flatten into manageable waves, and the impulsive reactions that once derailed their lives are replaced by intentional responses.
The Evidence for Long-Term Remission
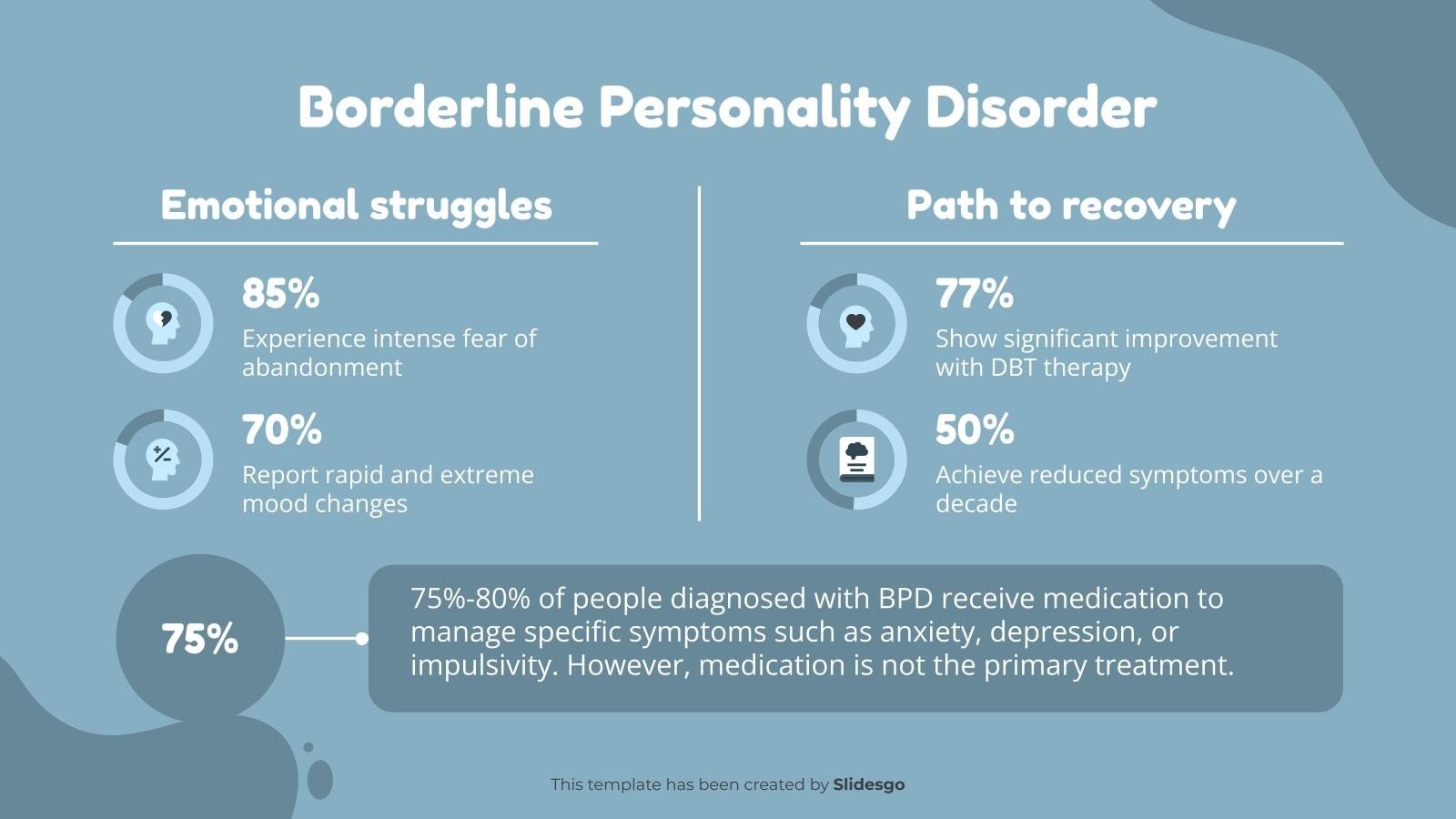
For decades, the medical community viewed BPD as a static condition. That narrative was dismantled by landmark longitudinal studies, most notably those conducted at the McLean Hospital. Research tracking patients over a decade found that a significant majority of people diagnosed with BPD eventually achieved remission. Specifically, studies have shown that up to 86% of patients no longer met the diagnostic criteria for BPD after ten years of follow-up via the National Center for Biotechnology Information.
Crucially, this remission often occurs even without intensive specialized treatment, though the speed and stability of recovery are significantly enhanced by professional intervention. The data suggests that the “worst” of the symptoms—such as self-harm and acute impulsivity—tend to decline more rapidly than the more enduring challenges, like chronic feelings of emptiness or interpersonal sensitivity.
This trajectory indicates that BPD is often a disorder of “emotional maturity” and regulation skills rather than a fixed biological defect. As individuals age and develop better cognitive coping mechanisms, the intensity of the disorder naturally tends to wane, a phenomenon that provides a critical glimmer of hope for those in their twenties who feel trapped by their diagnosis.
The Gold Standard: Dialectical Behavior Therapy (DBT)
If the data provides the hope, Dialectical Behavior Therapy (DBT) provides the toolkit. Developed by psychologist Marsha Linehan, DBT was specifically engineered to treat the chronic suicidality and emotional instability associated with BPD. Unlike traditional talk therapy, which may focus on the “why” of a patient’s history, DBT focuses on the “how” of their current survival.
DBT operates on the principle of “dialectics”—the idea that two opposite things can be true at once. In this case, the patient is accepted exactly as they are, while simultaneously being pushed to change the behaviors that are causing them pain. The therapy typically breaks down into four key modules designed to build psychological stability:
- Mindfulness: Learning to be present in the moment without judgment, reducing the tendency to spiral into past trauma or future anxiety.
- Distress Tolerance: Developing the ability to survive a crisis without making it worse through impulsive actions.
- Emotion Regulation: Identifying and labeling emotions to reduce vulnerability to “emotional hijackings.”
- Interpersonal Effectiveness: Learning how to ask for needs and set boundaries without damaging relationships.
By treating these skills as a “muscle” that can be trained, DBT transforms the experience of BPD from an uncontrollable storm into a manageable set of symptoms. The National Institute of Mental Health emphasizes the importance of integrated treatment plans that combine these behavioral skills with a supportive environment.
Defining the Path to Stability
Recovery from Borderline Personality Disorder does not indicate the person becomes a different version of themselves; rather, it means they gain the agency to choose how they respond to their feelings. This distinction is vital for those seeking support, as it removes the pressure to “fix” their personality and instead focuses on managing their reactions.
The process of recovery generally follows a pattern of stabilization, skill acquisition, and eventually, integration. The following table outlines the typical shift in experience as a person moves from acute BPD toward remission:
| Symptom Area | Acute Phase (Crisis) | Remission Phase (Recovery) |
|---|---|---|
| Emotional Response | Overwhelming, sudden “storms” | Manageable waves of emotion |
| Relationships | Idealization and devaluation | Stable, bounded connections |
| Impulse Control | Reactive, high-risk behaviors | Pause-and-reflect decision making |
| Self-Image | Fragmented or nonexistent | Consistent, integrated identity |
While the “emotional skin” of someone in recovery may always be thinner than that of a neurotypical person, the difference lies in the armor they have built. Recovery is characterized by the ability to feel a powerful emotion and recognize it as a feeling, rather than an absolute truth.
Navigating the Challenges of the Journey
Despite the positive statistics, the road to recovery is fraught with setbacks. The “fear of abandonment”—a hallmark of BPD—can often sabotage the very therapeutic relationships needed for healing. Patients may push away therapists or support systems during a crisis, which can lead to a renewed sense of hopelessness.
Mental health professionals suggest that the key to overcoming these plateaus is “radical acceptance.” By accepting that setbacks are a part of the process rather than a sign of failure, patients can avoid the shame-spiral that often triggers a relapse into old coping mechanisms. Community support, whether through peer groups or structured outpatient programs, serves as a critical buffer against the isolation that fuels the disorder.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Always seek the advice of a physician or other qualified health provider with any questions you may have regarding a medical condition.
If you or a loved one are experiencing a mental health crisis, please contact the 988 Suicide & Crisis Lifeline by calling or texting 988 in the US and Canada, or calling 111 in the UK.
The next milestone in the treatment of BPD is the increasing integration of digital health tools and “just-in-time” DBT interventions, which provide real-time coping strategies via smartphones during moments of acute distress. As these technologies evolve, the gap between clinical sessions and real-world application is expected to close, further increasing the rates of long-term stability for those affected.
We invite you to share your thoughts or experiences with recovery in the comments below, or share this guide with someone who may be seeking a path forward.
Worth a look