

For decades, a persistent statistical trend has suggested that women hold a biological advantage in longevity. While it is true that women generally live longer than men, a critical gap remains in the quality of those additional years. This phenomenon—where women live longer but not in better health—is not merely a biological quirk, but the result of systemic failures in how medical science is researched, practiced, and delivered.
From the chronic underrepresentation of women in clinical trials to the tendency of physicians to dismiss female pain as “emotional,” the medical field has historically operated on a male-centric model. As a board-certified physician, I have seen how this “gender data gap” translates into real-world consequences: delayed diagnoses, incorrect treatments, and a healthcare system that often views women’s health through the narrow lens of reproductive capacity rather than holistic well-being.
The disparity is most evident in the “morbidity-mortality paradox.” Women experience higher rates of non-fatal chronic conditions—such as autoimmune diseases and depression—and spend a larger proportion of their later years living with disability compared to men. This gap in health-adjusted life expectancy suggests that while the clock keeps ticking, the quality of life for many women is compromised by a system that fails to recognize their specific physiological and psychological needs.
The Danger of the ‘Male Default’ in Medical Research
The foundation of modern medicine is built on clinical trials, yet for years, these trials predominantly featured male subjects. The rationale was often based on the perceived “complication” of fluctuating female hormones, which researchers argued could skew data. In reality, this created a dangerous default where drugs and dosages were calibrated for the average man, then applied to women without sufficient validation.
This lack of sex-disaggregated data leads to significant risks in drug safety and efficacy. Women are more likely to experience adverse drug reactions as their metabolic rates, body composition, and hormonal profiles differ from men’s. When women are excluded from the initial phases of research, the medical community is essentially guessing how a treatment will affect half the population.
The impact extends beyond pharmaceuticals to the very way diseases are identified. For example, cardiovascular disease is often framed as a “man’s disease.” However, women frequently present with “atypical” symptoms—such as nausea, jaw pain, or extreme fatigue—rather than the classic crushing chest pain associated with male infarcts. Because the gold standard for diagnosis was built around male presentation, women are more likely to be misdiagnosed or sent home from emergency rooms during active cardiac events.
Beyond Fertility: The Narrow Scope of Women’s Health
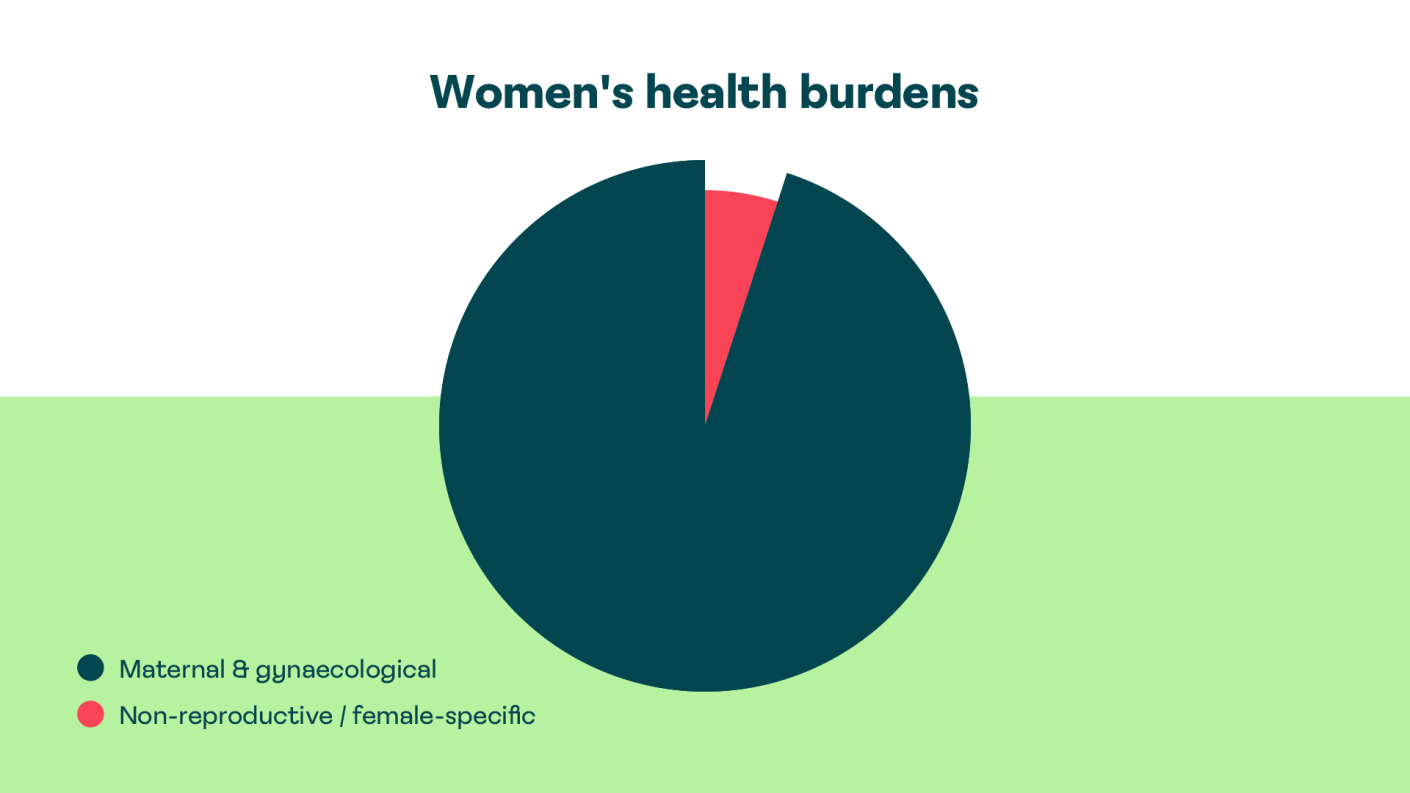
A recurring struggle for women in the healthcare system is the reduction of their medical identity to their reproductive organs. There is a pervasive institutional tendency to conflate “women’s health” exclusively with obstetrics and gynecology. This narrow focus means that conditions affecting women’s general health are often overlooked or attributed to the “natural” processes of menstruation or menopause.
This reductionist approach manifests in several critical areas:
- Pain Management: Studies and patient reports consistently indicate that women’s reports of pain are taken less seriously than men’s, often being labeled as “anxiety” or “psychosomatic.”
- Autoimmune Prevalence: Women are disproportionately affected by autoimmune disorders, such as lupus and rheumatoid arthritis, yet these conditions often take years to diagnose due to a lack of gender-specific diagnostic urgency.
- Mental Health: While women are diagnosed with depression and anxiety at higher rates, the underlying systemic drivers—such as the “double burden” of professional and domestic labor—are rarely addressed as clinical factors.
When the medical gaze is limited to fertility, the transition into menopause is often treated as a deficiency to be managed rather than a complex physiological shift requiring comprehensive care. This gap in understanding leaves millions of women struggling with symptoms that impact their cognitive function, bone density, and cardiovascular health.
The Systemic Burden of Care
The health disparity is not only clinical but structural. Women globally perform the vast majority of unpaid care function, acting as the primary caregivers for children, the elderly, and the sick. This “care penalty” creates a cycle of chronic stress and sleep deprivation that erodes long-term health.
This burden is compounded by economic disparities. Women are more likely to work in precarious, low-paying sectors with limited access to health insurance or paid sick leave. When a woman’s health is compromised, she often delays seeking care to prioritize the needs of her dependents, further delaying diagnosis and worsening the prognosis of treatable conditions.
| Factor | Impact on Women’s Health | Resulting Outcome |
|---|---|---|
| Clinical Trial Bias | Underrepresentation of female biology | Higher rates of adverse drug reactions |
| Symptom Misinterpretation | Reliance on “male-standard” symptoms | Delayed diagnosis of heart disease/stroke |
| Reproductive Reductionism | Health viewed through fertility lens | Neglect of non-reproductive chronic illness |
| Caregiving Burden | Chronic stress and unpaid labor | Higher morbidity in later life |
Moving Toward Gender-Informed Medicine
Closing the health gap requires a fundamental shift from “gender-blind” medicine to “gender-informed” care. This begins with mandatory sex-disaggregated data in all clinical research, as advocated by organizations like the World Health Organization (WHO), ensuring that the efficacy of a treatment is proven for all bodies, not just the male average.
Medical education must likewise evolve. Training for future physicians needs to emphasize the diversity of symptom presentation and challenge the implicit biases that lead clinicians to dismiss female patients. Recognizing that a woman’s health is not defined by her uterus is the first step toward a system that treats the whole person.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition.
The path forward involves a rigorous application of the “Gender Lens” across public health policy. The next critical step in this evolution is the increasing adoption of mandates requiring the inclusion of women in all phases of clinical trials, a movement currently gaining traction in regulatory frameworks globally. As these mandates move from recommendations to requirements, the medical community will finally initiate to bridge the gap between living longer and living well.
We want to hear from you. Have you experienced a delay in diagnosis or felt dismissed by a healthcare provider? Share your experience in the comments below or share this article to help raise awareness about the gender data gap.