

Restoring mobility after a severe tendon injury is often a grueling process, but for one patient facing the rare challenge of a bilateral simultaneous chronic Achilles tendon rupture, a combination of traditional and minimally invasive surgery provided a path back to walking. The case highlights a sophisticated surgical approach using the transfer of the flexor hallucis longus (FHL) tendon to replace the function of the Achilles, which is the strongest tendon in the human body.
The Achilles tendon is critical for plantar flexion—the action of pointing the foot downward—which allows a person to push off the ground while walking or running. When this tendon ruptures and remains untreated for an extended period, it becomes a “chronic” rupture. In such cases, the tendon ends often retract and atrophy, making a simple primary repair impossible because there is no longer enough healthy tissue to sew back together.
This specific medical case involved a patient who suffered from these ruptures in both legs simultaneously. Because the injuries were chronic, surgeons had to look beyond standard repair techniques, opting instead for a bilateral simultaneous chronic Achilles tendon rupture treated with open and endoscopic flexor hallucis longus tendon transfer. This procedure essentially “borrows” a nearby tendon to do the job of the damaged Achilles.
As a physician, I find this case particularly noteworthy because it demonstrates the evolution of orthopedic surgery—specifically the move toward hybrid techniques that combine the visibility of open surgery with the precision and faster recovery times of endoscopic procedures.
Understanding the FHL Tendon Transfer
The flexor hallucis longus (FHL) is the muscle and tendon responsible for flexing the big toe. While essential for balance, it is not as critical for walking as the Achilles. In a tendon transfer, the FHL is rerouted from its original path and attached to the calcaneus (heel bone), effectively taking over the role of the missing Achilles tendon.
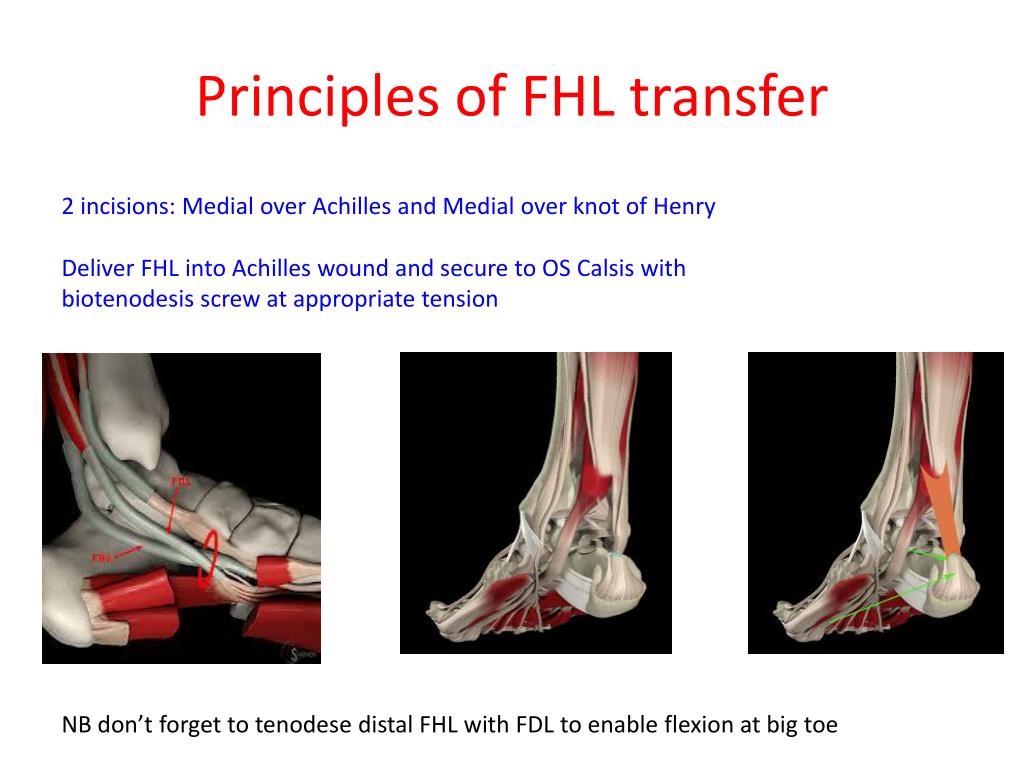
In this patient’s case, the surgical team employed a dual approach. On one side, an open surgical technique was used, providing the surgeon with a direct view of the anatomy to ensure secure fixation. On the other, an endoscopic approach was utilized. Endoscopic surgery involves using a small camera and specialized tools through tiny incisions, which typically results in less tissue trauma, reduced postoperative pain, and a lower risk of infection.
The goal of this combined approach is to maximize the stability of the transfer while minimizing the overall surgical burden on a patient who is already facing a complex recovery process in both limbs.
The Surgical Timeline and Recovery Process
Recovering from bilateral surgery is significantly more complex than recovering from a unilateral (single-sided) injury. The patient cannot simply lean on one “good” leg while the other heals. This requires a highly coordinated rehabilitation strategy to prevent muscle atrophy and joint stiffness.
The progression of recovery generally follows a strict clinical sequence:
- Immediate Post-Operative Phase: Immobilization in a cast or boot to allow the transferred tendon to integrate and heal into the bone.
- Controlled Weight-Bearing: A gradual transition from non-weight-bearing to partial weight-bearing, often using walkers or crutches to avoid putting too much tension on the new graft.
- Physical Therapy: Focused exercises to regain the range of motion in the ankle and strengthen the calf muscles.
- Functional Return: The eventual transition back to independent walking and daily activities.
| Feature | Open Surgery | Endoscopic Surgery |
|---|---|---|
| Visibility | Direct, wide-field view | Magnified, camera-guided view |
| Incision Size | Larger, traditional incision | Small “keyhole” portals |
| Tissue Trauma | Higher potential for scarring | Minimal soft-tissue disruption |
| Recovery Speed | Standard healing timeline | Often faster initial recovery |
Why This Case Matters for Public Health
Chronic Achilles ruptures are often the result of delayed diagnosis or failed initial treatments. When both legs are affected, the impact on a patient’s quality of life is profound, leading to a total loss of independent mobility. This case serves as a clinical blueprint for treating “hopeless” chronic ruptures where the original tendon is completely gone.
The use of the Achilles tendon repair protocols usually focuses on acute injuries. But, the shift toward FHL transfers for chronic cases represents a critical alternative. By utilizing the FHL, surgeons can restore a significant percentage of the original push-off strength, which is the difference between a patient requiring a wheelchair and a patient being able to walk independently.
the integration of endoscopic techniques reflects a broader trend in orthopedic surgery toward “minimally invasive” interventions. Reducing the size of the surgical wound is not just about aesthetics; it reduces the risk of wound dehiscence (opening of the surgical site), which is a known complication in lower-limb surgeries due to poor blood flow in the ankle region.
Challenges and Constraints
While the outcome in this case was positive, FHL transfers are not without trade-offs. The most notable is the loss of independent big toe flexion. While most patients find this a negligible loss compared to the ability to walk, it can affect certain athletic activities. The success of the surgery is heavily dependent on the quality of the remaining FHL tendon; if that tendon is also diseased or ruptured, other grafts (such as the posterior tibial tendon) must be considered.
The “simultaneous” nature of the bilateral surgery also increases the anesthetic risk and the complexity of postoperative nursing care. Managing two surgical sites while ensuring the patient does not develop deep vein thrombosis (DVT)—a common risk in lower-limb immobilization—requires vigilant medical monitoring.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Please consult a board-certified orthopedic surgeon or healthcare provider for diagnosis and treatment of tendon injuries.
The next phase for patients undergoing these complex transfers is typically a long-term follow-up to assess the durability of the transfer and the return of muscle strength. Clinical monitoring usually continues for one to two years post-surgery to ensure the graft remains stable under the stresses of daily ambulation.
Do you have experience with tendon recovery or questions about minimally invasive orthopedic surgery? We invite you to share your thoughts and experiences in the comments below.