

Medical science has long understood the mechanics of why older adults fall and how to prevent them. From the degradation of muscle mass to the subtle shift in vestibular balance, the clinical blueprints for safety are well-documented. Yet, there remains a persistent and dangerous gap between this clinical knowledge and the actual implementation of falls prevention in daily life.
For many seniors, a single trip or slip is not merely an accident but a catalyst for a rapid decline in independence. The fear of falling often leads to a self-imposed restriction of activity, which paradoxically increases the risk of future falls by accelerating muscle atrophy and joint stiffness. Closing the gap in falls prevention requires moving beyond generic advice and toward personalized, sustainable interventions that integrate into a person’s existing routine.
The challenge is not a lack of data, but a lack of translation. While healthcare providers can identify risk factors—such as polypharmacy, poor lighting, or declining vision—the transition from a doctor’s recommendation to a modified home environment or a consistent exercise regimen is where the system often fails. Effective prevention must address the psychological barriers and systemic hurdles that prevent seniors from adopting life-saving changes.
The Multifactorial Nature of Fall Risks
Falls are rarely the result of a single cause. Instead, they typically occur when multiple risk factors converge. According to the Centers for Disease Control and Prevention (CDC), falls are the leading cause of injury-related deaths among adults aged 65 and older, often involving a combination of intrinsic biological changes and extrinsic environmental hazards.
Intrinsic factors include the natural loss of bone density and muscle strength, known as sarcopenia, and the onset of chronic conditions like Parkinson’s disease or diabetic neuropathy, which can numb the feet and distort a person’s sense of where they are in space. Extrinsic factors are often the “low-hanging fruit” of prevention: loose rugs, inadequate lighting in hallways, and the absence of grab bars in bathrooms.
A critical but often overlooked factor is medication. Many common prescriptions, including sedatives, antidepressants, and certain blood pressure medications, can cause dizziness or drowsiness. When a patient is taking five or more medications—a common scenario in geriatric care—the risk of an adverse drug interaction that leads to a fall increases significantly.
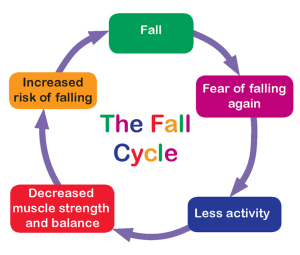
The Psychological Cycle of Fear
One of the most complex hurdles in falls prevention is the “fear of falling” (FOF) cycle. When an older adult experiences a fall, the resulting trauma often triggers a behavioral shift. To avoid another incident, they may stop walking to the park, avoid visiting friends, or cease light housework. This avoidance leads to physical deconditioning, which weakens the core and legs, ultimately making a future fall more likely.
Breaking this cycle requires a shift in perspective: moving from a philosophy of “avoiding risk” to one of “building resilience.” The goal is not to eliminate every possible hazard—which is impossible—but to ensure the body is strong enough and the environment is safe enough to manage the risks of daily living.
Translating Knowledge Into Action
Turning clinical evidence into a lived reality requires a multidisciplinary approach. It is no longer sufficient for a primary care physician to simply suggest “staying active.” Instead, a coordinated effort involving physical therapists, occupational therapists, and family members is necessary to create a sustainable safety plan.

Strength and balance training, particularly programs that emphasize leg strength and proprioception (the body’s ability to sense its location, movements, and actions), have proven most effective. Tai Chi, for example, is frequently cited in clinical literature as a gold-standard intervention for improving balance and reducing fall frequency among the elderly.
| Risk Category | Common Trigger | Actionable Intervention |
|---|---|---|
| Physical | Muscle weakness/Poor balance | Strength training & Tai Chi |
| Environmental | Clutter/Poor lighting | Home safety assessment & LED upgrades |
| Medical | Medication side effects | Comprehensive medication review |
| Sensory | Vision or hearing loss | Annual eye exams & hearing aids |
Beyond exercise, the “home audit” is a critical tool. An occupational therapist can identify specific “danger zones” in a residence. Simple changes, such as removing throw rugs or installing a higher-seated toilet, can drastically reduce the likelihood of a catastrophic event. However, these changes must be implemented with the individual’s consent and preference to ensure they are maintained.
Systemic Barriers to Prevention
Despite the availability of these strategies, systemic gaps remain. In many healthcare systems, falls prevention is treated as a reactive measure—something addressed after a hip fracture—rather than a proactive part of primary care. There is often a lack of integrated billing or insurance coverage for comprehensive home safety assessments, meaning only those with the financial means can access professional modifications.
there is a societal tendency to view the decline of balance as an inevitable part of aging. This “ageist” narrative can discourage seniors from seeking aid, as they may perceive that their loss of mobility is simply “how it is” rather than a treatable medical condition. Reframing balance as a skill that can be maintained and improved is essential for patient engagement.
For those seeking further guidance on evidence-based strategies, the National Institute on Aging (NIA) provides comprehensive resources on how to conduct home safety checks and identify high-risk medications.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition.
The next phase of falls prevention is expected to integrate wearable technology and AI-driven gait analysis, which can alert caregivers to subtle changes in a person’s walking pattern before a fall occurs. These tools aim to move the needle from general prevention to predictive intervention, allowing for “just-in-time” support that preserves autonomy while ensuring safety.
We invite you to share your experiences with home safety or questions about balance in the comments below.