

Recognizing the early warning signs of colorectal cancer can be the difference between a routine procedure and a complex medical battle. Whereas many of the symptoms are subtle and can be easily mistaken for common digestive issues, a persistent change in bowel habits or the appearance of blood in the stool warrants immediate medical attention.
As a physician and medical writer, I often encounter patients who hesitate to report these changes, fearing a worst-case scenario or assuming the symptoms are merely the result of aging or diet. However, colorectal cancer is highly treatable when caught early, and the most critical step in the process is the transition from noticing a symptom to scheduling a clinical evaluation.
The challenge lies in the fact that colon cancer often develops silently. Many patients are asymptomatic in the early stages, which is why the medical community has shifted its focus toward aggressive screening. Understanding the specific colon cancer symptoms and the risk factors associated with them allows patients to advocate for their own health before a condition progresses.
When symptoms do appear, they typically manifest as changes in the digestive tract’s function. These may include a persistent change in bowel habits—such as diarrhea, constipation, or narrowing of the stool—that lasts for more than a few days. The most urgent red flag is rectal bleeding or blood in the stool, which can appear bright red or dark and tarry.
Identifying Red Flags and Risk Factors
Not every digestive upset indicates malignancy, but certain patterns are more concerning than others. Ongoing digestive symptoms that do not resolve with simple dietary changes should be discussed with a healthcare professional. A doctor will look for a combination of symptoms, such as unexplained weight loss, fatigue caused by anemia, and a feeling that the bowel does not empty completely.
During an initial consultation, a physician will conduct a detailed review of a patient’s medical history to identify specific risk factors. Some factors are non-modifiable, such as age and genetics, while others are related to lifestyle choices. A family history of colorectal cancer or the presence of precancerous polyps significantly increases a person’s risk profile.
Medical professionals also monitor for chronic inflammatory bowel diseases (IBD), including Crohn’s disease and ulcerative colitis, as these conditions cause long-term inflammation of the digestive tract, which can increase the likelihood of developing cancer over time.
Lifestyle factors also play a measurable role. Research indicates that obesity, a sedentary lifestyle with low physical activity, heavy alcohol consumption, and smoking are all linked to a higher incidence of the disease. Identifying these markers early helps doctors determine how aggressively a patient needs to be monitored.
The Diagnostic Pathway: From Exam to Biopsy
Once a patient reports concerning symptoms, the diagnostic process follows a specific sequence designed to rule out benign causes and identify malignancies. The first step is typically a physical examination, which may include a digital rectal exam. In this procedure, a doctor uses a gloved, lubricated finger to feel for abnormalities or masses in the rectum.
Depending on the findings, the physician may order preliminary tests. These often include blood tests to check for anemia or fecal tests to detect occult blood—blood that is not visible to the naked eye. If these tests return abnormal results, or if the clinical suspicion remains high, a diagnostic colonoscopy is the gold standard for next steps.
A colonoscopy is performed by a gastroenterologist who uses a colonoscope—a long, flexible tube equipped with a light and a tiny video camera—to examine the entire lining of the colon and rectum. This is not only a diagnostic tool but also a therapeutic one. if the doctor finds a suspicious growth or a polyp, they can remove the tissue immediately for a biopsy.
The biopsy is the final and most definitive step. A pathologist examines the removed tissue under a microscope to determine if cancer cells are present and, if so, what type of colorectal cancer it is. This pathological confirmation dictates the entire treatment plan moving forward.
Screening Guidelines and Timelines
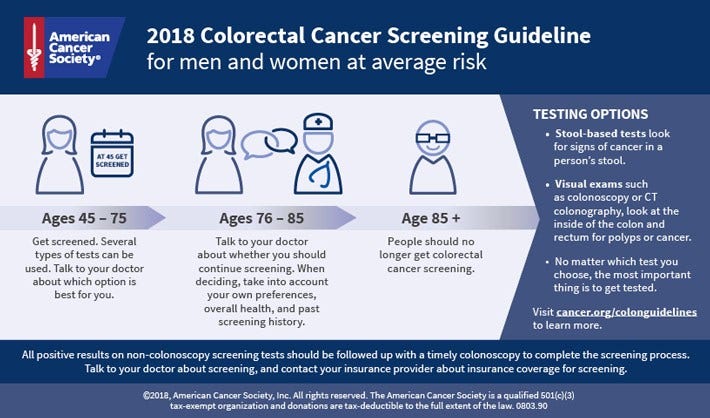
Because symptoms often appear only after the cancer has progressed, screening is the most effective way to prevent the disease. For individuals at average risk, the current medical consensus is to begin regular screening at age 45. However, those with a family history or personal history of polyps must often start much earlier.
| Test Type | Recommended Frequency | Methodology |
|---|---|---|
| Colonoscopy | Every 10 years | Visual exam of the entire colon |
| Stool-based Tests | Every 1 to 3 years | Detection of blood or DNA markers |
| CT Colonography | Every 5 years | Radiological imaging of the colon |
| Sigmoidoscopy | Every 5 years | Visual exam of the lower colon |
The choice of test often depends on the patient’s preference and their specific risk factors. While stool-based tests are less invasive, a colonoscopy remains the only method that allows for the simultaneous detection and removal of precancerous polyps, effectively stopping cancer before it starts.
Why Early Detection Matters
The impact of early detection cannot be overstated. When colorectal cancer is found in its earliest stages, the survival rates are significantly higher, and the treatment options are often less invasive. Conversely, waiting for severe colon cancer symptoms to appear can mean the disease has spread to lymph nodes or other organs, complicating the recovery process.
For those at increased risk—including people with hereditary syndromes like Lynch syndrome or FAP—the timeline for screening is accelerated. In these cases, doctors may recommend screenings every one to two years rather than the standard decade. This proactive approach transforms the disease from a potential crisis into a manageable health condition.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition.
The next major checkpoint for public health officials and medical providers will be the continued monitoring of the “early-onset” trend, as colorectal cancer rates continue to rise in adults under 50. Updated guidelines from the National Cancer Institute and other health bodies will continue to refine screening ages based on new population data.
Do you have questions about screening or a personal story about early detection? Share your thoughts in the comments below or share this guide with a loved one.