

For many women, the transition into menopause brings a sense of closure to a specific chapter of reproductive health. Even though, for some, a forgotten piece of medical history can resurface decades later in the form of alarming symptoms. When a post-menopausal woman experiences unexpected vaginal bleeding, the immediate clinical concern is often malignancy, but the cause can sometimes be a retained Lippes Loop IUD—a contraceptive device inserted years, or even decades, prior.
Post-menopausal bleeding is treated as a medical red flag. In the clinical world, any bleeding after the cessation of menstruation is considered abnormal until proven otherwise, as it can be an early warning sign of endometrial hyperplasia or uterine cancer. Yet, in a subset of cases, the culprit is not a disease, but a “forgotten” intrauterine device (IUD) that has remained embedded in the uterine wall, triggering chronic inflammation and erratic bleeding.
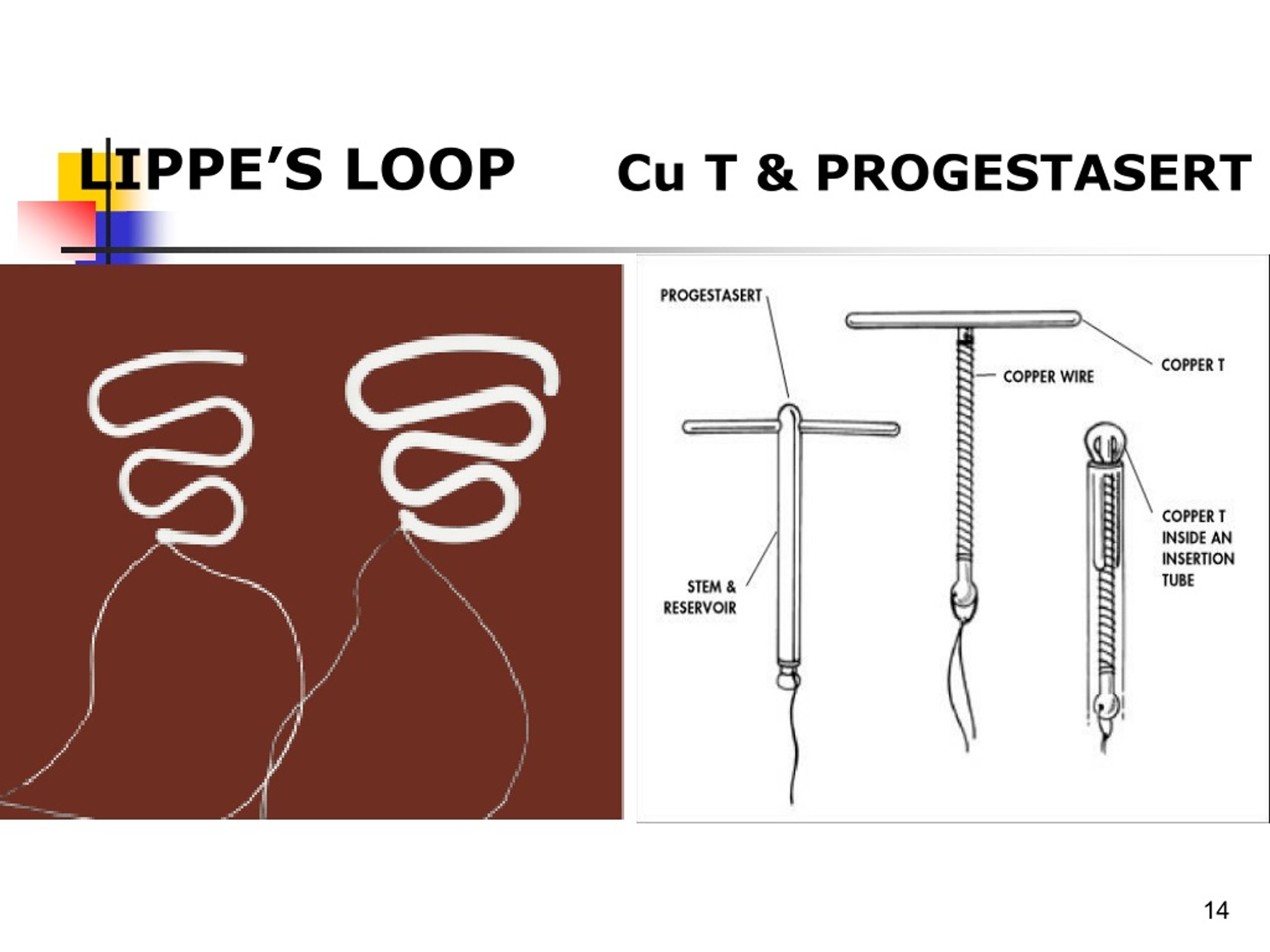
The Lippes Loop, specifically, represents an older era of reproductive medicine. Unlike modern hormonal or copper IUDs, the Lippes Loop was a non-medicated, inert plastic device. While largely phased out in developed nations by the 1980s, these devices were designed to be long-term, and in some instances, they were never removed, remaining silent and invisible within the uterus for a lifetime.
The Legacy of the Non-Medicated IUD
To understand why a retained Lippes Loop causes issues in later life, it is necessary to glance at the device’s design. The Lippes Loop was a first-generation IUD made of polyethylene. It worked primarily by creating a foreign-body reaction within the endometrium, which prevented pregnancy. Because it lacked the specialized coatings of modern devices, it relied entirely on its shape and the body’s inflammatory response to be effective.
Over time, these devices can shift or develop into “embedded,” meaning the plastic arms of the loop migrate into the myometrium (the muscular wall of the uterus). When a woman reaches menopause, the uterine lining thins significantly due to the drop in estrogen. This atrophy can change the relationship between the device and the uterine wall, potentially leading to the erosion of the lining or the development of polyps, which manifests as post-menopausal bleeding.
Chronic pelvic pain is another hallmark of a retained foreign body. The constant presence of an inert object can lead to low-grade, chronic inflammation or, in some cases, the formation of adhesions. For the patient, this often feels like a dull, persistent ache in the lower abdomen that may be dismissed as general aging or arthritis until a gynecological exam reveals the truth.
Diagnosing a Forgotten Foreign Body
The challenge in diagnosing a retained Lippes Loop is that the patient may have forgotten the device existed, or the original provider may not have documented its insertion. This leaves the physician to solve a diagnostic puzzle based on symptoms alone. The process typically follows a specific clinical sequence:
- Patient History: A detailed review of contraceptive history, though this is often unreliable if the device was inserted decades ago.
- Transvaginal Ultrasound: This is the gold standard for initial screening. A transvaginal ultrasound can typically visualize the high-density plastic of the IUD against the softer uterine tissue.
- Hysteroscopy: If imaging is inconclusive but bleeding persists, a doctor may leverage a hysteroscope—a thin, lighted tube—to look directly inside the uterine cavity.
- Endometrial Biopsy: Because bleeding in menopause is so closely linked to cancer, a biopsy is almost always performed simultaneously to rule out malignancy before the IUD is removed.
Comparison of IUD Generations
| Device Type | Material/Mechanism | Common Era | Primary Risk of Retention |
|---|---|---|---|
| Lippes Loop | Inert Polyethylene | 1960s–1980s | Embedding in uterine wall |
| Copper IUD | Plastic with Copper Wire | 1980s–Present | Perforation or displacement |
| Hormonal IUD | Levonorgestrel-releasing | 1990s–Present | String loss/migration |
The Path to Resolution
Once a retained Lippes Loop is identified, the primary goal is removal to alleviate pain and stop the bleeding. Because these older devices often lack the retrieval strings found on modern IUDs, removal can be more complex. Surgeons typically use a combination of hysteroscopy and specialized grasping forceps to extract the device. In rare cases where the loop is deeply embedded in the uterine muscle, a minor surgical procedure called a myomectomy may be required to retrieve the plastic.
The relief following removal is often immediate regarding the pelvic pain, though the bleeding may take a short time to resolve as the endometrium heals. The discovery of a retained IUD often serves as a reminder of the importance of comprehensive medical records. As patients move between providers over several decades, a “forgotten” procedure from 1975 can become a medical mystery in 2024.
For women experiencing any form of post-menopausal bleeding, the priority remains a swift evaluation by a healthcare provider. While the discovery of a retained IUD is a benign outcome compared to the alternative of uterine cancer, the symptoms are identical, making professional screening non-negotiable.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition.
Medical professionals continue to monitor long-term outcomes for patients with first-generation IUDs. The next step for those experiencing unexplained pelvic symptoms is typically a referral to a gynecological specialist for advanced imaging and potential hysteroscopic intervention.
Do you or a loved one have a history of early contraceptive use? Share your thoughts or questions in the comments below.