

For decades, the medical community viewed certain cancers as inevitable tragedies of biology. But the introduction of the human papillomavirus (HPV) vaccine has fundamentally shifted that narrative, offering the first and only tool capable of preventing multiple types of cancer before they ever have a chance to develop.
Despite its potential, HPV vaccine access and use in the U.S. remains a complex puzzle of public health success and systemic failure. While the vaccine has evolved to cover more strains and requires fewer doses, the path to immunization is often blocked by regional disparities, vaccine hesitancy, and a persistent gap in care for the most vulnerable populations.
As a physician, I have seen how a simple series of shots in early adolescence can effectively erase a lifetime of cancer risk. Yet, the transition from clinical efficacy to universal protection is rarely linear. In the U.S., the story of the HPV vaccine is not just one of medical triumph, but of the ongoing struggle to ensure that life-saving prevention reaches every zip code, regardless of race or income.
The Hidden Burden: HPV and Cancer Trends
Human papillomavirus is the most common sexually transmitted infection in the United States. It is so prevalent that approximately 42.5 million Americans are currently infected, with at least 13 million new infections occurring annually. While most HPV infections resolve on their own, persistent high-risk strains can trigger cellular changes that lead to malignancy.
The impact is most visible in cervical cancer, where over 90% of cases are directly linked to HPV. Strains 16 and 18 alone are responsible for roughly 66% of these cases worldwide. However, the burden of the disease is not shared equally. A stark paradox exists in the U.S. Healthcare system: Black and Hispanic women often have the highest rates of recent Pap testing, yet Black women face the highest mortality rates from cervical cancer.
This disparity suggests that screening alone is not a cure for systemic inequality. Factors such as delayed follow-up treatment after abnormal results, diagnosis at later stages of disease progression, and negative experiences within the medical system contribute to a disproportionate death toll among women of color.
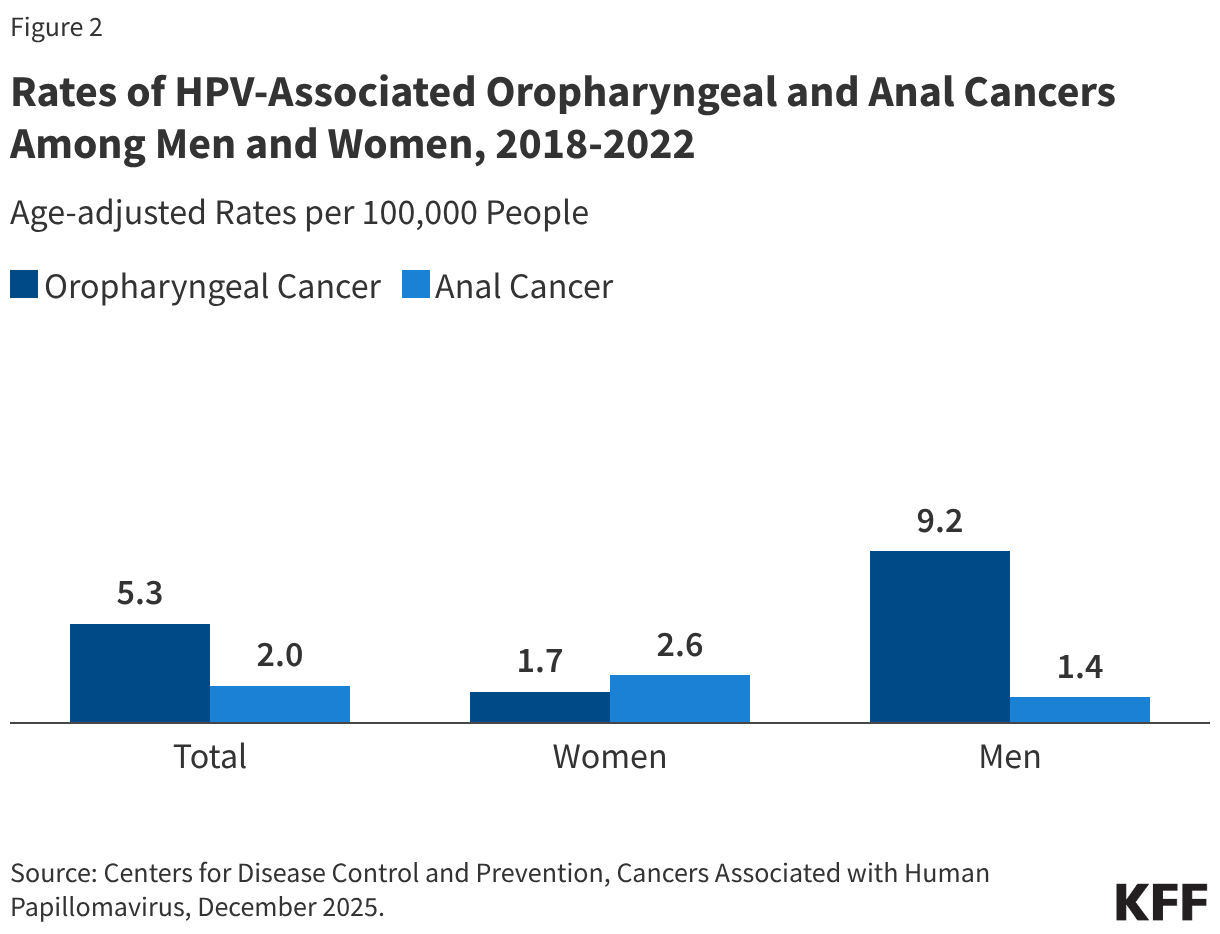
While cervical and vaginal cancer rates have trended downward since 1999, other HPV-related cancers are on the rise. Oropharyngeal (throat) cancers have develop into the most common HPV-associated malignancy among men, with roughly 70% of these cases attributed to the virus. Similarly, HPV is responsible for 91% of the estimated 7,600 annual cases of anal cancer in the U.S.
The Evolution of the HPV Vaccine
Since 2016, Gardasil 9 has been the sole HPV vaccine available in the U.S. Unlike earlier versions, this vaccine protects against nine different strains of the virus, covering the majority of cases related to cervical, anal, and throat cancers, as well as genital warts. Originally marketed primarily for young women, the recommendation has since expanded to include boys, young men, and people of all genders, recognizing that HPV is a universal health risk.
Current guidelines from the Advisory Committee on Immunization Practices (ACIP) emphasize the importance of timing. The vaccine is most effective when administered before the initiation of sexual activity. For most adolescents, this means a two-dose series. While the vaccine cannot treat an existing HPV infection, it remains beneficial for those already infected by protecting them against other strains they have not yet encountered.
The longevity of this protection is a key point of reassurance for parents and clinicians. Data indicates that the vaccine’s effectiveness remains strong for more than 10 years, with no evidence of waning protection. In Scotland, for example, a program targeting 12- and 13-year-olds resulted in zero cases of cervical cancer among the fully vaccinated cohort since the program’s inception in 2008.
The Access Gap: State and Socioeconomic Barriers
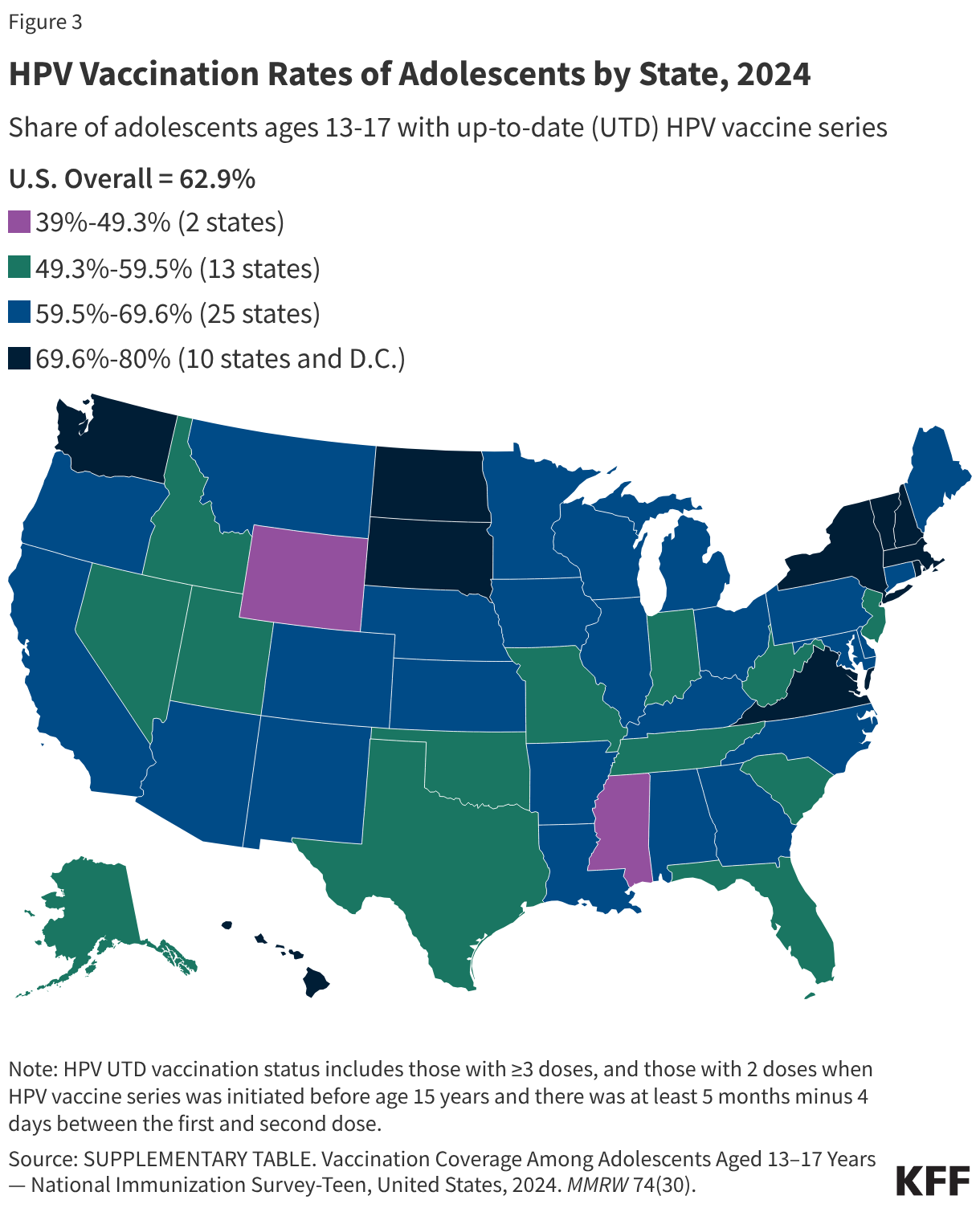
Despite the availability of the vaccine, uptake is uneven. In 2024, over 60% of adolescents aged 13-17 were up-to-date with their HPV vaccinations. However, this number masks deep geographic and social divides. Vaccination rates range from a low of 39% in Mississippi to a high of 80% in Massachusetts.
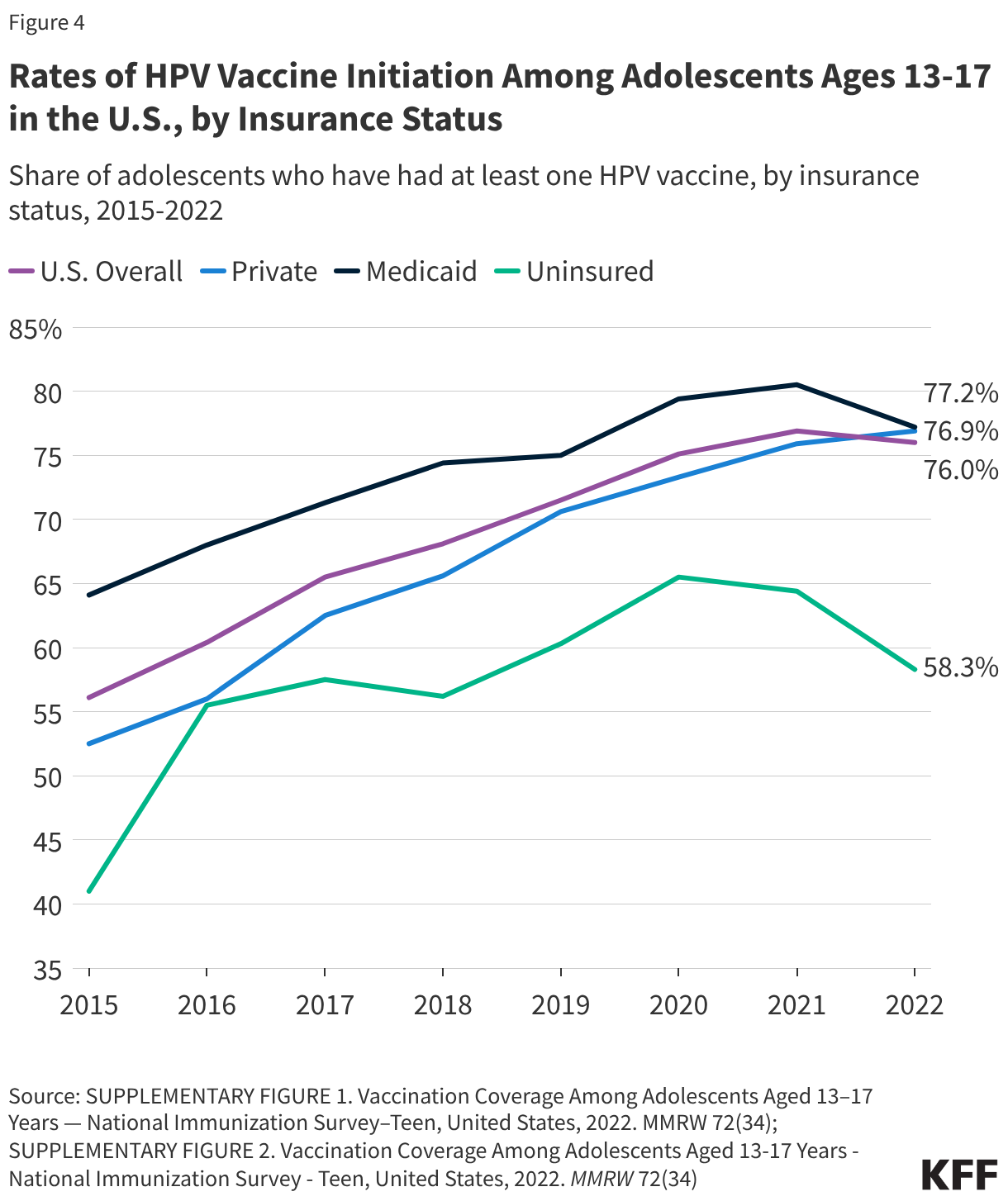
Rural residents continue to face lower vaccination rates than their urban counterparts, often due to limited provider access and transportation hurdles. While many adolescents start the vaccine series, a significant number never complete it. In 2024, roughly 79% of girls and 77% of boys received at least one dose, but completion rates lag behind.
Vaccine hesitancy has also intensified since the COVID-19 pandemic. Providers report an increase in parents citing safety concerns or the belief that the vaccine is unnecessary. Research shows that the single most effective way to combat this hesitancy is a direct recommendation from a healthcare provider; children are significantly more likely to be vaccinated when their doctor explicitly advises their parents to do so.
Removing the Financial Barrier
Cost should not be a deterrent to cancer prevention. Under the Affordable Care Act (ACA), most private and public insurance plans are required to cover ACIP-recommended immunizations, including the HPV vaccine, without consumer cost-sharing. For those without traditional insurance, several safety nets exist:
- Vaccines for Children (VFC): A CDC-funded program providing vaccines at no cost to children who are uninsured, underinsured, or Medicaid-eligible.
- Medicaid: Covers recommended vaccines for enrolled individuals under age 21 through the EPSDT program.
- Section 317: Federal grants provided to state and local agencies to extend vaccine availability to uninsured adults.
- Patient Assistance: The manufacturer, Merck, offers assistance programs to provide free vaccines to low-income, uninsured adults aged 19 and older.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Please consult a licensed healthcare provider for personalized medical recommendations.
The next major milestone in the fight against HPV-related cancers will be the continued monitoring of long-term vaccine efficacy and the potential for streamlined delivery systems to reach rural populations. As public health officials work to close the gap in racial and geographic disparities, the goal remains clear: a future where HPV-related cancers are a rarity rather than a risk.
Do you have questions about the HPV vaccine or your family’s immunization schedule? Share your thoughts in the comments or share this article with others to help spread awareness.