

Medical researchers are refining the approach to treating babesiosis, a tick-borne illness that can cause severe anemia and systemic complications, particularly in vulnerable populations. Recent clinical observations and studies are focusing on optimizing drug combinations to ensure faster clearance of the parasite and a reduction in relapse rates, which have historically complicated the recovery process for patients.
Babesiosis is caused by Babesia parasites, which infect and destroy red blood cells. While many healthy adults experience mild, flu-like symptoms, the condition can be life-threatening for elderly patients, those with compromised immune systems, or individuals with asplenia (the absence of a functioning spleen). The urgency for a more refined babesiosis treatment protocol stems from the parasite’s ability to linger in the body, necessitating precise dosing and duration of therapy to prevent recurrence.
The current gold standard for treatment typically involves a combination of atovaquone and azithromycin. However, the medical community continues to evaluate the efficacy of these regimens against varying strains of the parasite and the impact of patient-specific comorbidities. By analyzing patient outcomes and parasite loads, clinicians are working to move toward a more personalized medicine approach that balances aggressive eradication with the minimization of drug toxicity.
Understanding the Pathology of Babesia Infection
Unlike Lyme disease, which is caused by bacteria, babesiosis is caused by protozoa. These organisms enter the bloodstream via the bite of an infected Ixodes tick and specifically target erythrocytes. This leads to hemolytic anemia, where the body destroys its own red blood cells faster than it can produce them.
The challenge for physicians is that the symptoms—fever, chills, and fatigue—overlap significantly with other tick-borne illnesses and common viral infections. This often leads to diagnostic delays. Once identified, the treatment goal is not only to alleviate symptoms but to completely clear the parasite from the blood to avoid the “latent” phase, where the infection can resurface months or years later.
Who is most at risk?
While anyone spending time in wooded or grassy areas in endemic regions can contract the parasite, certain groups face higher stakes:
- Asplenic Individuals: Because the spleen is primary in filtering out damaged red blood cells and parasites, those without a spleen are at high risk for severe, rapid-onset disease.
- The Elderly: Age-related declines in immune function can make it harder for the body to fight the infection without aggressive pharmaceutical intervention.
- Immunocompromised Patients: Those undergoing chemotherapy or living with HIV may experience prolonged infections that require extended courses of medication.
Evaluating Treatment Efficacy and Protocols
The shift in recent study focus has been toward the “duration of therapy.” Historically, treatment lengths were standardized, but data suggests that some patients require longer courses to achieve complete parasitologic cure. The use of clindamycin in combination with quinine has been a long-standing alternative, though it is often associated with more significant side effects than the atovaquone-azithromycin pairing.
Clinicians now emphasize the importance of monitoring the “parasite load” through repeated blood smears or PCR (polymerase chain reaction) testing. This allows doctors to determine if the babesiosis treatment is working in real-time or if a change in medication is required to prevent a relapse.
| Drug Combination | Primary Use Case | Common Considerations |
|---|---|---|
| Atovaquone + Azithromycin | First-line therapy for most adults | Generally better tolerated; shorter course |
| Clindamycin + Quinine | Severe cases or resistant strains | Higher toxicity; requires closer monitoring |
| Exchange Transfusion | Critical, life-threatening anemia | Used in hospital settings to stabilize oxygen |
The Role of Diagnostics in Treatment Success
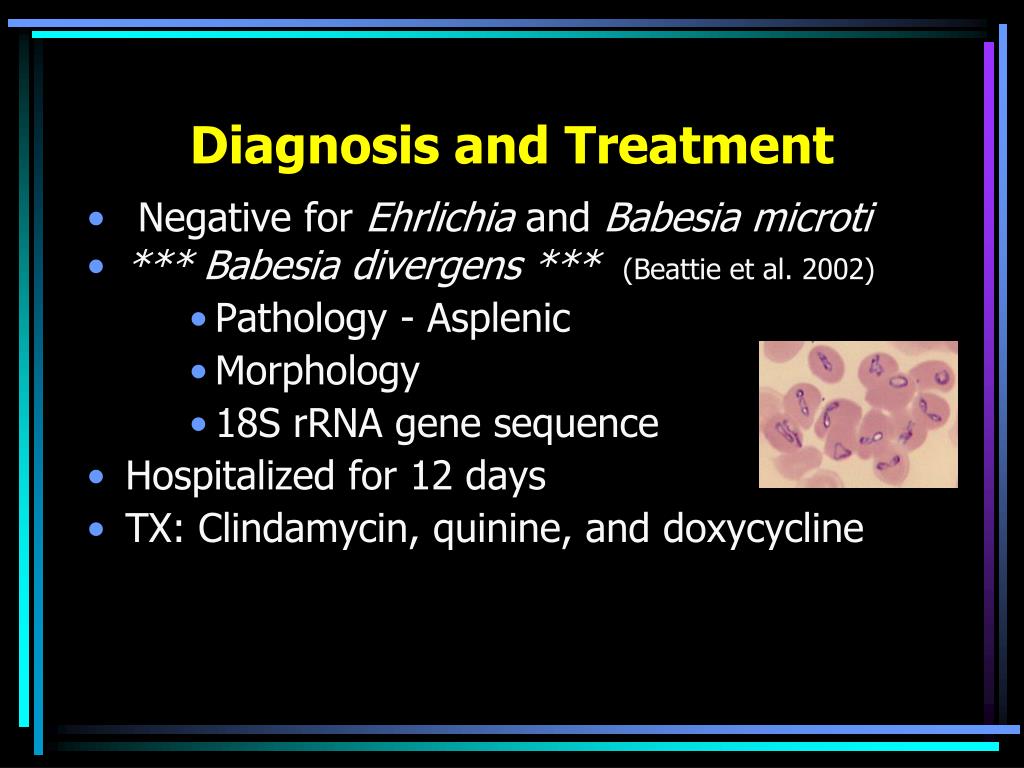
The success of any pharmacological intervention depends entirely on the speed and accuracy of the initial diagnosis. The “gold standard” remains the microscopic examination of a Giemsa-stained blood smear, where clinicians look for the characteristic “Maltese cross” formation of the parasites within red blood cells.
However, because the parasite count can fluctuate, a single negative test does not always rule out the infection. The integration of molecular diagnostics, such as PCR testing, has significantly increased the sensitivity of detection, allowing for earlier intervention and better long-term outcomes.
When treatment begins early, the risk of severe complications—such as acute respiratory distress syndrome (ARDS) or multi-organ failure—is drastically reduced. This highlights the necessity of “geographic suspicion,” where doctors maintain a high index of suspicion for babesiosis in patients presenting with fever who have a history of travel to endemic areas like the Northeast or Upper Midwest of the United States.
Looking Forward: Next Steps in Tick-Borne Research
The medical community is currently looking toward the development of more targeted therapies that can eliminate the parasite without the systemic side effects associated with current antimicrobial combinations. Research is also expanding into the understanding of “co-infections,” as many patients are bitten by ticks carrying both Babesia and Borrelia burgdorferi (Lyme disease) simultaneously.
The next major checkpoint in this field will be the publication of larger, multi-center longitudinal studies that track patients over several years post-treatment. These studies aim to define the exact threshold of parasite clearance required to guarantee that a patient is truly cured and will not suffer a relapse.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition.
We invite readers to share their experiences with tick-borne illness recovery or ask questions about current diagnostic trends in the comments below.