
A rare genetic disorder, retinal vasculopathy with cerebral leukoencephalopathy and systemic manifestations (RVCL-S), can sometimes mimic a brain tumor, presenting a diagnostic challenge for physicians. This was the case with a patient recently reported in a case study, highlighting the importance of thorough investigation and immunological monitoring in individuals with this condition.
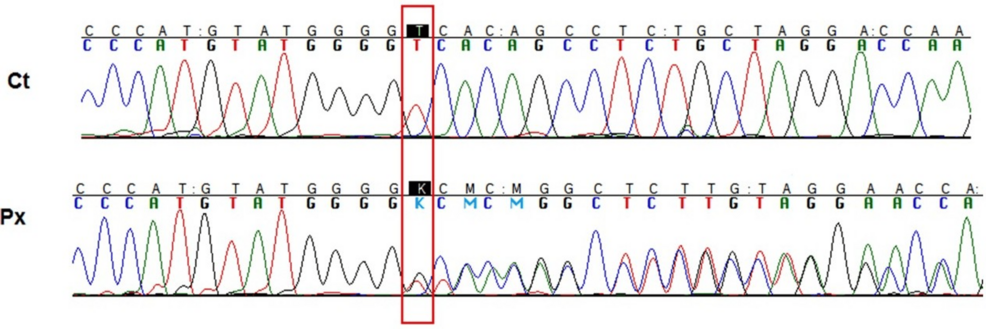
RVCL-S is a microvascular disorder caused by mutations in the TREX1 gene, impacting protein localization and leading to a range of systemic issues. The condition is autosomal dominant, meaning only one copy of the mutated gene is needed to cause the disorder. The case, detailed in a report published by Cureus, involved a patient carrying a common TREX1 variant, NM_033629.6:c.703dup (p.Val235fs), who exhibited the classic symptoms of RVCL-S alongside unusual pulmonary granulomatous lesions suggestive of sarcoidosis. This expanded the known spectrum of how RVCL-S can manifest.
Diagnostic Challenges and the Role of Genetic Testing
The initial presentation of RVCL-S can be particularly deceptive, as the cerebral manifestations can closely resemble those of a brain tumor. Accurate diagnosis relies heavily on genetic testing to identify the TREX1 mutation. Early and precise identification is crucial, not only for the patient but also for family members, as the condition is inherited. The case report underscores the need for clinicians to consider RVCL-S in the differential diagnosis of patients presenting with neurological symptoms and retinal vasculopathy.
Transcriptomic analysis performed on the patient and his pre-symptomatic daughter, who also carried the same TREX1 variant, revealed a mild upregulation of inflammatory signaling pathways. This suggests that even before symptoms appear, there’s an underlying inflammatory process at play. This finding supports the idea that proactive monitoring of asymptomatic carriers could be beneficial.
Treatment Approaches and Ongoing Research
Currently, there is no cure for RVCL-S. Treatment focuses on managing symptoms and slowing disease progression. In the reported case, the patient was treated with a Janus kinase (JAK) inhibitor. Although there was a period of initial clinical stabilization, the patient ultimately experienced disease progression. This highlights the complexities of managing RVCL-S and the need for further research into effective therapies. Research published in PubMed emphasizes the importance of targeted therapy in addressing this rare condition.
The use of JAK inhibitors, while showing some initial promise, requires careful consideration. The case report suggests that the response to treatment can be transient, and ongoing monitoring is essential. Further investigation is needed to determine the optimal dosage, duration, and patient selection criteria for JAK inhibitor therapy in RVCL-S.
Systemic Manifestations Beyond the Brain and Retina
RVCL-S is not limited to neurological and ophthalmological symptoms. The case report highlights the potential for systemic involvement, specifically the development of pulmonary granulomatous lesions resembling sarcoidosis. This underscores the importance of a comprehensive clinical evaluation, including assessment of other organ systems, in patients suspected of having RVCL-S. The systemic nature of the disease necessitates a multidisciplinary approach to care, involving neurologists, ophthalmologists, pulmonologists, and immunologists.
The Importance of Immunological Monitoring
The researchers emphasize the critical role of systematic immunological monitoring in individuals with RVCL-S, even those who are currently asymptomatic. The mild upregulation of inflammatory signaling pathways observed in the pre-symptomatic daughter suggests that early intervention may be possible. Regular monitoring can help identify subtle changes in immune function that may precede the onset of clinical symptoms, allowing for timely initiation of treatment or preventative measures.
The case report also highlights the need for clinical surveillance of asymptomatic carriers. This includes regular neurological examinations, ophthalmological assessments, and monitoring for other systemic manifestations. By closely tracking the clinical course of these individuals, researchers can gain a better understanding of the natural history of RVCL-S and identify potential targets for therapeutic intervention.
As research continues, a deeper understanding of the underlying mechanisms driving RVCL-S will be crucial for developing more effective treatments. The case presented serves as a reminder of the diagnostic challenges posed by this rare disorder and the importance of a collaborative, multidisciplinary approach to patient care. The authors declared no conflicts of interest in their research, as noted in the PubMed abstract.
The next step in understanding and treating RVCL-S will likely involve larger-scale studies to validate the findings of this case report and to explore the potential of novel therapeutic strategies. Continued research and clinical surveillance are essential for improving the lives of individuals affected by this challenging condition.
Have thoughts on this story? Share your comments below.