

Most of us have lived through it: the jittery anticipation before a major presentation, the haze of a cross-continental flight, or the restlessness of a high-stakes exam. A few nights of poor sleep are usually a temporary frustration, a glitch in the system that corrects itself once the stress subsides. But for a significant portion of the population, the system doesn’t reset.
For approximately 10 percent of adults, the struggle to find rest becomes a daily battle. In these cases, a handful of sleepless nights turn into insomnia, creating a self-perpetuating cycle where the fear of not sleeping becomes the very thing that keeps the brain wired.
As a physician, I often see patients who view insomnia simply as a nighttime problem. However, clinical sleep medicine treats it as a comprehensive 24-hour disorder. The primary indicator isn’t just what happens between 11 p.m. And 6 a.m., but how the lack of restoration impairs a person’s ability to function during the day.
Defining the threshold of insomnia
There is a critical distinction between “bad sleep” and clinical insomnia. According to Wendy Troxel, an American sleep scientist, the diagnosis relies heavily on daytime limitations. When sleep deficiency begins to erode cardiovascular health, immune function, and emotional stability, it moves from a nuisance to a medical condition.
The psychological component is equally vital. Jamie Zeitzer, co-director of the Center for Sleep and Circadian Science at Stanford University, notes that the level of distress is a primary diagnostic criterion. If a person takes 30 minutes to fall asleep but feels relaxed and unaffected, they likely do not have insomnia. The disorder manifests when that same 30-minute window triggers anxiety, creating a state of hyper-arousal.
Clinically, sleep issues are categorized by their duration and frequency:
- Acute Insomnia: Short-term sleep loss often triggered by life events. Symptoms typically include daytime fatigue, irritability, memory lapses, and mood swings.
- Chronic Insomnia: This represents diagnosed when sleep disturbances occur at least three nights per week for three months or longer, provided the symptoms aren’t caused by another medical condition or substance utilize.
The biological trap: Why the brain stays awake
Logically, a night of total sleep deprivation should create the following night’s sleep effortless. However, the human brain does not always follow this linear path. Some individuals experience what is known as paradoxical hyperactivity.
In this state, the brain attempts to compensate for extreme sleepiness by artificially boosting alertness. Instead of crashing, the system over-corrects, making it even harder to drift off the next night. This biological misfire is often fueled by a failure of the body to “downshift.”
Raj Dasgupta, a sleep physician at Huntington Memorial Hospital in California, explains that insomnia keeps cortisol levels and sympathetic nervous system activity elevated during the night—times when they should naturally plummet. Essentially, the body remains in a state of “fight or flight” whereas lying in bed, preventing the deep restoration required for systemic health.
The psychological loop and environmental triggers
Beyond biology, the brain is a powerful associative machine. When a person spends multiple nights lying awake in frustration, the bedroom ceases to be a sanctuary of rest and instead becomes a trigger for stress. The brain begins to associate the bed with wakefulness and anxiety rather than sleep.
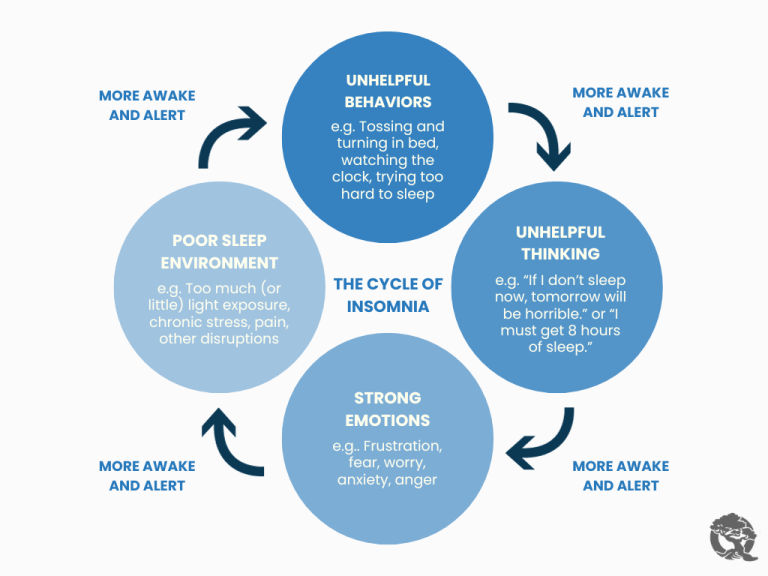
This associative learning is a primary driver of chronic cases. Research from Sweden found that 91 percent of people with insomnia exhibited anxiety and maladaptive sleep habits specifically linked to their sleep environment. The bed becomes a place of mental labor—calculating how many hours of sleep are left before the alarm goes off—which further spikes arousal levels.
Long-term systemic consequences
The risks of untreated chronic insomnia extend far beyond morning grogginess. The most immediate danger is the development of psychiatric disorders. A long-term study conducted by Johns Hopkins University followed more than 1,000 young men for over 30 years, finding that chronic sleep deficiency significantly increased the risk of developing clinical depression.
The impact on physical health is equally concerning. Recent research from 2025 suggests a strong link between chronic insomnia and increased cardiovascular and metabolic risks. The persistent elevation of stress hormones can lead to systemic inflammation, a higher risk of type 2 diabetes, and diminished immune response.
there is emerging evidence regarding brain health. Chronic sleep loss is increasingly connected to impaired cognitive function and a higher long-term risk of neurodegenerative diseases, as the brain’s natural “cleaning” process—the removal of metabolic waste—is most efficient during deep sleep.
Breaking the cycle: The path to recovery
The good news is that insomnia is highly treatable. The clinical “gold standard” is Cognitive Behavioral Therapy for Insomnia (CBT-I). Unlike sedative medications, which treat the symptom, CBT-I addresses the underlying behavioral and thought patterns that maintain the disorder.
To begin reprogramming the brain, experts recommend a strict adherence to “stimulus control” and sleep hygiene:
- The Sleep-Only Rule: Go to bed only when you are actually sleepy. If you cannot fall asleep within a reasonable timeframe, receive out of bed and move to another room. This breaks the association between the bed and frustration.
- Consistent Scheduling: Maintain a rigorous wake-up time, regardless of how much sleep you achieved the night before.
- The Wind-Down Ritual: Establish a structured, relaxing routine. This includes limiting blue light from screens, avoiding caffeine in the late afternoon, and engaging in calming activities like meditation or a warm bath.
| Feature | Acute Insomnia | Chronic Insomnia |
|---|---|---|
| Duration | Days to weeks | 3+ months |
| Frequency | Occasional/Event-driven | 3+ nights per week |
| Primary Driver | External stressor | Biological/Psychological loop |
| Main Risk | Short-term cognitive lag | Metabolic & Psychiatric disorders |
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition.
As research into circadian science evolves, the focus is shifting toward personalized sleep medicine. Future updates in the field are expected to provide more nuanced markers for identifying those most susceptible to the transition from acute sleep loss to chronic insomnia, allowing for earlier intervention before the associative loop takes hold.
Do you struggle with the “wired but tired” feeling? Share your experiences or questions in the comments below.