

For patients living with macular telangiectasia type 2 (MacTel), a rare degenerative eye disease that erodes central vision, the search for a treatment that preserves retinal health without causing significant harm has been a long-standing clinical challenge. Novel data suggests a potential breakthrough in this effort, as a ciliary neurotrophic factor drug well-tolerated in MacTel patients has demonstrated a favorable safety profile in recent clinical evaluations.
The drug, known as Ciliary Neurotrophic Factor (CNTF), is designed to provide neuroprotection to the retinal ganglion cells and other neurons in the eye. Unlike many current treatments for retinal diseases that focus on reducing swelling or leaking blood vessels, CNTF aims to support the survival of existing neurons, potentially slowing the progression of the vision loss associated with MacTel.
As a physician, I have seen how the anxiety of “treatment-induced complications” often weighs as heavily on patients as the disease itself. The latest findings indicate that the administration of this neurotrophic factor was well-tolerated, meaning the incidence of severe adverse events was low and the drug did not trigger the inflammatory responses that often plague intravitreal injections.
Understanding the Mechanism of Neuroprotection
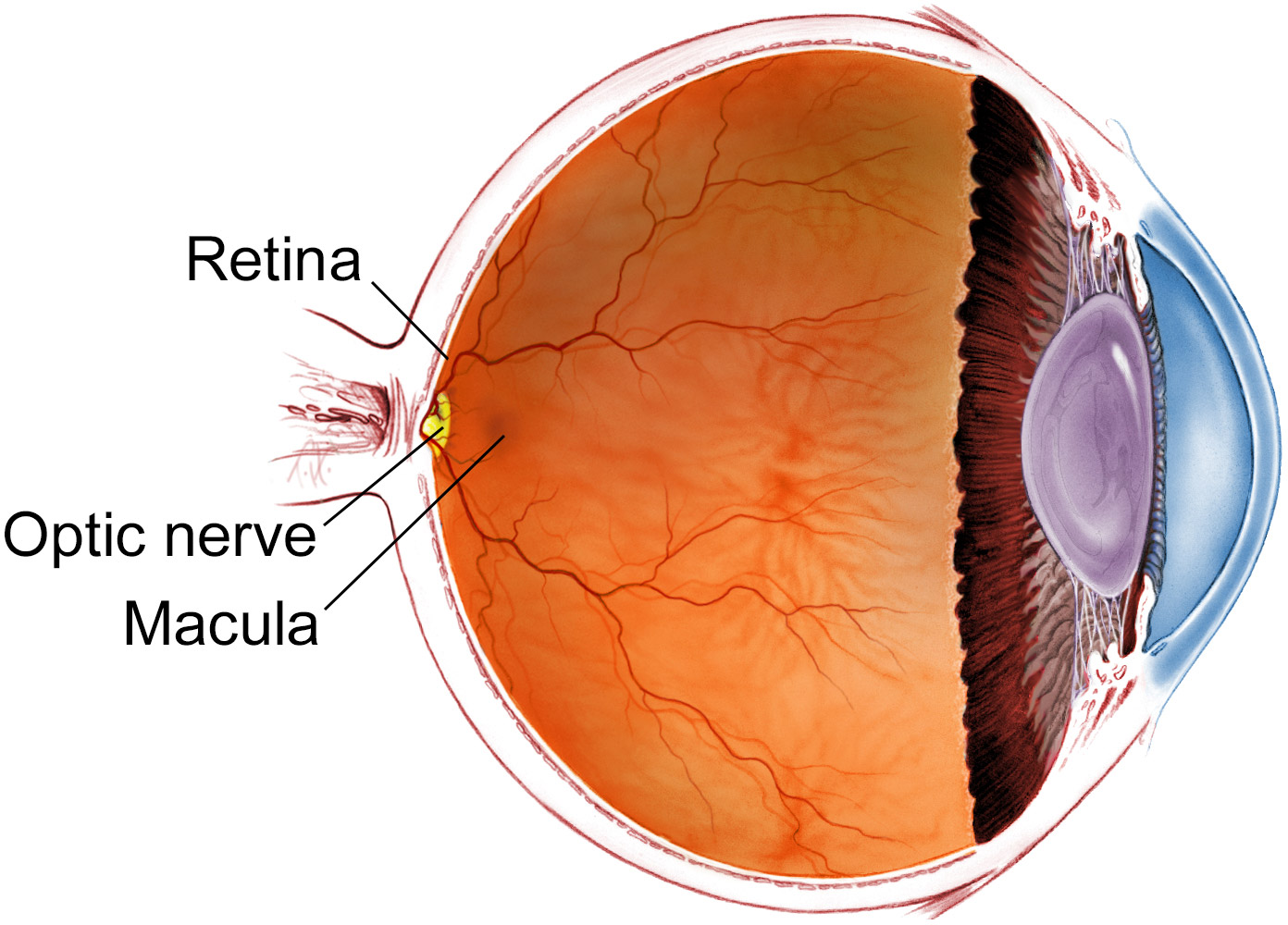
MacTel is characterized by the gradual loss of neurons and the breakdown of the retinal architecture, leading to “holes” in the central vision. This process is not merely about vascular leakage but involves a fundamental failure of the cells to survive. This is where Ciliary Neurotrophic Factor comes into play. By mimicking the natural proteins that keep neurons alive, the drug seeks to stabilize the retinal environment.
The clinical focus has shifted toward “neuroprotection”—the idea that we can shield the remaining healthy cells from the toxic environment created by the disease. The recent data confirms that the drug can be delivered into the vitreous of the eye without causing significant toxicity or systemic side effects, a critical hurdle for any drug intended for long-term chronic use.
The primary goal of this therapy is to prevent the atrophy of the macula, the part of the eye responsible for sharp, central vision. By maintaining the integrity of the retinal layers, clinicians hope to preserve the ability of patients to read, drive, and recognize faces, which are the first functions typically lost in MacTel progression.
The Significance of Tolerability in Retinal Therapy
In the world of ophthalmology, “tolerability” is not just a buzzword; It’s a matter of safety. Any drug injected into the eye carries risks, ranging from endophthalmitis (infection) to an increase in intraocular pressure. The fact that the CNTF drug was well-tolerated suggests that the molecular structure of the factor does not provoke an aggressive immune response within the ocular chamber.
For patients, this means a lower likelihood of needing rescue medications or facing complications that could further jeopardize their remaining vision. When a drug is well-tolerated, it allows researchers to focus on the efficacy—whether it actually stops the disease—without the noise of severe side effects clouding the data.
The study’s findings are particularly encouraging because MacTel patients often have fragile retinal structures. A drug that is gentle on the tissue even as providing a biological “shield” represents a significant shift from the aggressive anti-VEGF therapies used in other macular diseases, which may not be as effective or appropriate for the unique pathology of MacTel.
Comparing Treatment Approaches
To understand why the tolerability of CNTF is so vital, it is helpful to compare it to the standard of care for other retinal conditions. While MacTel is distinct, many patients are mistakenly treated with therapies designed for wet AMD (Age-related Macular Degeneration).
| Approach | Primary Goal | Mechanism | Typical Patient Profile |
|---|---|---|---|
| Anti-VEGF | Reduce Leakage | Blocks blood vessel growth | Wet AMD / Diabetic Macular Edema |
| Neuroprotection (CNTF) | Cell Survival | Supports neuronal health | MacTel / Degenerative Retinopathies |
| Surgical Intervention | Structural Repair | Physical stabilization | Retinal Detachment / Macular Holes |
The shift toward neuroprotection acknowledges that once a neuron is dead, it cannot be brought back. The “window of opportunity” for a drug like CNTF is most open in the early to mid-stages of the disease, where the drug can act as a preservative for the remaining cellular architecture.
What This Means for the Patient Journey
For the average person diagnosed with MacTel, the news of a well-tolerated neuroprotective drug provides a roadmap for future care. However, it is important to distinguish between tolerability and cure. The data confirms the drug is safe to use; the next critical phase is proving that it significantly alters the clinical trajectory of the disease over several years.
Those affected by MacTel often face a “diagnostic odyssey,” where they are misdiagnosed with other forms of macular degeneration. The development of targeted therapies like CNTF encourages more precise diagnostic protocols, as the benefit of the drug is tied specifically to the neurodegenerative nature of MacTel.
The current timeline for these treatments involves moving from safety trials (Phase I/II) into larger efficacy trials (Phase III). The confirmation that the drug is well-tolerated is the “green light” needed to proceed with larger cohorts of patients, which will eventually lead to regulatory review and, if successful, clinical availability.
Remaining Constraints and Unknowns
Despite the optimism, several questions remain. The long-term durability of the neuroprotective effect is still being studied. Because retinal degeneration happens over decades, a few months of data cannot fully predict whether the drug will prevent blindness over a ten-year period. The optimal dosing frequency—how often a patient must receive an injection—remains a key variable that will determine the practical utility of the treatment.
There is too the question of patient selection. Not all MacTel patients progress at the same rate. Identifying the specific biomarkers that indicate who will respond best to CNTF is the next frontier for the researchers involved in these trials.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Patients should consult with a board-certified ophthalmologist or retina specialist regarding treatment options for Macular Telangiectasia.
The next major milestone for this therapy will be the publication of long-term efficacy data from expanded clinical trials, which will determine if the safety of the drug is matched by a meaningful preservation of visual acuity. Updates on these trials are typically shared through the National Library of Medicine’s clinical trials database.
We invite you to share your thoughts or questions about new retinal therapies in the comments below, or share this article with others who may be affected by MacTel.
Worth a look