

For many, the first signs of chronic venous disease appear as a minor annoyance: a feeling of heaviness in the legs after a long day or the appearance of compact, spider-like veins on the surface of the skin. However, these superficial changes often mask a more complex systemic failure of the circulatory system. When the valves in the leg veins fail to function correctly, blood pools in the lower extremities, creating a cascade of pressure that can lead to significant skin degradation and mobility issues.
Chronic venous disease (CVD) is a progressive condition that affects millions of adults globally. While often dismissed as a cosmetic concern due to the visibility of varicose veins, the pathology involves a breakdown of the venous walls and valves that are responsible for pushing blood upward toward the heart against the force of gravity. When these valves leak, a phenomenon known as venous reflux occurs, increasing the hydrostatic pressure within the veins.
As a board-certified physician, I have seen how the gap between the onset of symptoms and medical intervention can lead to preventable complications. Understanding the progression of chronic venous disease is essential for early diagnosis, as the condition typically evolves from simple swelling to permanent skin changes and, in severe cases, non-healing ulcers.
The Mechanics of Venous Insufficiency
To understand why CVD occurs, one must look at the “muscle pump” of the calf. In a healthy leg, the calf muscles contract during walking, squeezing the deep veins and pushing blood upward. One-way valves prevent the blood from flowing backward. In patients with venous insufficiency, these valves turn into incompetent. This failure allows blood to flow backward and pool in the lower legs, a state referred to as venous hypertension.
This increased pressure forces fluid and proteins out of the blood vessels and into the surrounding interstitial tissue, resulting in edema, or swelling. Over time, this chronic inflammation can cause the skin to thicken and discolor, a process known as stasis dermatitis. If the pressure remains unchecked, the skin may break down entirely, leading to venous stasis ulcers—open sores that are notoriously difficult to heal due to the fact that the compromised circulation prevents oxygen and nutrients from reaching the wound site.
Identifying the Stages of Progression
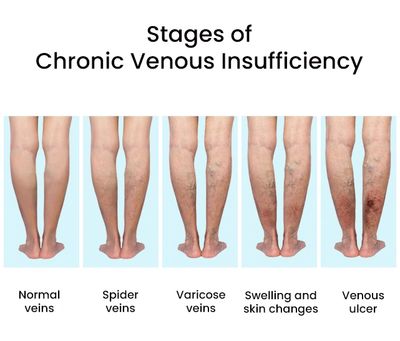
Medical professionals typically categorize the severity of the disease to determine the appropriate course of treatment. The progression is rarely sudden; it is a slow accumulation of damage that often goes unnoticed until the symptoms interfere with daily activity.
- Early Stage: Characterized by “heavy” legs, aching, or cramping, particularly after prolonged standing or sitting. Spider veins (telangiectasias) may appear.
- Moderate Stage: Visible varicose veins develop. Swelling (edema) becomes more pronounced, often disappearing overnight but returning during the day.
- Advanced Stage: The skin becomes hyperpigmented (brownish discoloration) and hardens. This is often accompanied by eczema or chronic skin inflammation.
- Critical Stage: The formation of venous ulcers, typically occurring around the ankles, which require specialized wound care to prevent infection.
Risk Factors and Vulnerable Populations
While genetics play a significant role—often inheriting a predisposition for weak valve walls—environmental and lifestyle factors significantly accelerate the onset of the disease. Prolonged standing or sitting without movement is one of the primary triggers, as it removes the mechanical assistance of the calf muscle pump.
Obesity increases the pressure on the pelvic and abdominal veins, further hindering the return of blood from the legs. Pregnancy causes both hormonal changes that relax vein walls and physical pressure from the growing uterus on the inferior vena cava, the body’s largest vein. Age is another critical factor, as the elasticity of the veins naturally decreases over time.
| Factor | Impact on Venous Health | Risk Level |
|---|---|---|
| Genetics | Inherited valve insufficiency | High |
| Prolonged Standing | Increased hydrostatic pressure | Moderate to High |
| Obesity | External compression of deep veins | Moderate |
| Advanced Age | Loss of vessel wall elasticity | High |
| Previous DVT | Permanent valve damage (Post-thrombotic syndrome) | Very High |
Modern Treatment and Management Strategies
The goal of treating chronic venous disease is to reduce venous pressure and improve blood flow. Management usually begins with conservative therapy, which focuses on lifestyle modifications and mechanical support. Compression therapy, using medical-grade stockings, is the gold standard for managing edema. These stockings apply graduated pressure, which helps squeeze blood back toward the heart and prevents fluid from leaking into the tissues.
For patients who do not respond to conservative measures, minimally invasive procedures have largely replaced traditional “vein stripping” surgeries. Endovenous Laser Ablation (EVLA) and Radiofrequency Ablation use heat to seal off the damaged vein, forcing the blood to reroute through healthier, functioning veins. These procedures are typically performed in an office setting with minimal downtime, allowing patients to return to activity quickly.
According to the Mayo Clinic, these interventions not only improve the aesthetic appearance of the legs but are critical in preventing the progression to ulceration. For those already suffering from ulcers, a combination of compression and specialized dressings is required to facilitate closure.
Practical Steps for Daily Prevention
Preventing the worsening of CVD involves breaking the cycle of venous stasis. Simple behavioral changes can significantly reduce the daily load on the venous system:
- Movement: Incorporating “walking breaks” every hour to engage the calf muscles.
- Elevation: Raising the legs above the level of the heart for 15–30 minutes several times a day to allow gravity to assist blood return.
- Weight Management: Reducing systemic pressure on the venous network through a balanced diet and exercise.
- Footwear: Avoiding high heels for extended periods, as they limit the full range of motion in the calf muscle.
For more detailed guidelines on vascular health and diagnostic criteria, the Society for Vascular Surgery provides clinical resources for patients and providers.
Disclaimer: This article is for informational purposes only and does not constitute professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition.
As research into vascular biology advances, the focus is shifting toward earlier screening and the use of ultrasound mapping to identify valve failure before skin changes occur. The next milestone in venous care involves the refinement of bio-engineered stents and more precise ablation techniques to minimize side effects. Patients experiencing persistent leg heaviness or swelling are encouraged to schedule a venous doppler ultrasound for an accurate baseline assessment.
Do you have experience managing venous health or questions about these treatments? Share your thoughts in the comments below or share this guide with someone who may be experiencing these symptoms.
Keep reading