

The rapid global response to the COVID-19 pandemic necessitated an unprecedented acceleration of clinical research, placing a spotlight on antiviral candidates that could reduce hospitalization and mortality. Among the most scrutinized was Remdesivir, a broad-spectrum antiviral originally developed for Ebola, which became a cornerstone of early efforts to treat the Wuhan coronavirus phase trials for Remdesivir and manage severe SARS-CoV-2 infections.
As a physician and medical writer, I have followed the trajectory of Remdesivir from its initial promise in laboratory settings to its complex journey through human clinical trials. The drug, an adenosine analog, was designed to inhibit the viral RNA polymerase, effectively “jamming” the machinery the virus uses to replicate within human cells. While its introduction provided a critical tool for clinicians, the data emerging from various global trials offered a nuanced picture of its efficacy.
The urgency of the pandemic led to the deployment of Remdesivir across multiple phases of testing, ranging from small-scale safety cohorts to massive randomized controlled trials. These efforts aimed to determine not only if the drug worked, but for whom it worked best and at what stage of the disease the intervention was most effective. The results fundamentally shifted the standard of care for hospitalized patients during the first two years of the pandemic.
The Clinical Evolution of Remdesivir
The transition from in vitro studies to human application was marked by a series of high-stakes trials. Early data suggested that Remdesivir could shorten the time to recovery in patients with COVID-19, particularly those requiring supplemental oxygen. However, the medical community remained cautious until large-scale, double-blind, placebo-controlled studies could verify these findings.
One of the most influential studies was the ACTT-1 trial, sponsored by the National Institute of Allergy and Infectious Diseases (NIAID). This study found that Remdesivir shortened the time to recovery in hospitalized adults, leading to the first FDA Emergency Apply Authorization (EUA). Despite this, other trials, such as the Solidarity trial led by the World Health Organization (WHO), suggested that the drug had little to no effect on overall mortality or the need for mechanical ventilation in the most severely ill patients.
This discrepancy highlighted a critical reality in pharmacological research: the timing of administration is everything. For patients in the early stages of pneumonia or respiratory distress, the antiviral could curb viral load; for those already in the midst of a cytokine storm (hyper-inflammation), the viral replication phase had often passed, making an antiviral less effective than corticosteroids like dexamethasone.
Comparing Trial Outcomes and Impact
To understand the impact of these trials, it is helpful to gaze at the primary endpoints measured across different study designs. The focus shifted from “complete recovery” to “time to clinical improvement” and “mortality rates.”
| Trial/Entity | Primary Focus | Key Finding |
|---|---|---|
| NIAID (ACTT-1) | Recovery Time | Shortened time to recovery in hospitalized patients. |
| WHO (Solidarity) | Mortality/Ventilation | Limited to no effect on 28-day mortality. |
| FDA Status | Regulatory Approval | Granted EUA and later full approval for adult/pediatric use. |
| Clinical Use | Standard of Care | Most effective when administered early in the disease course. |
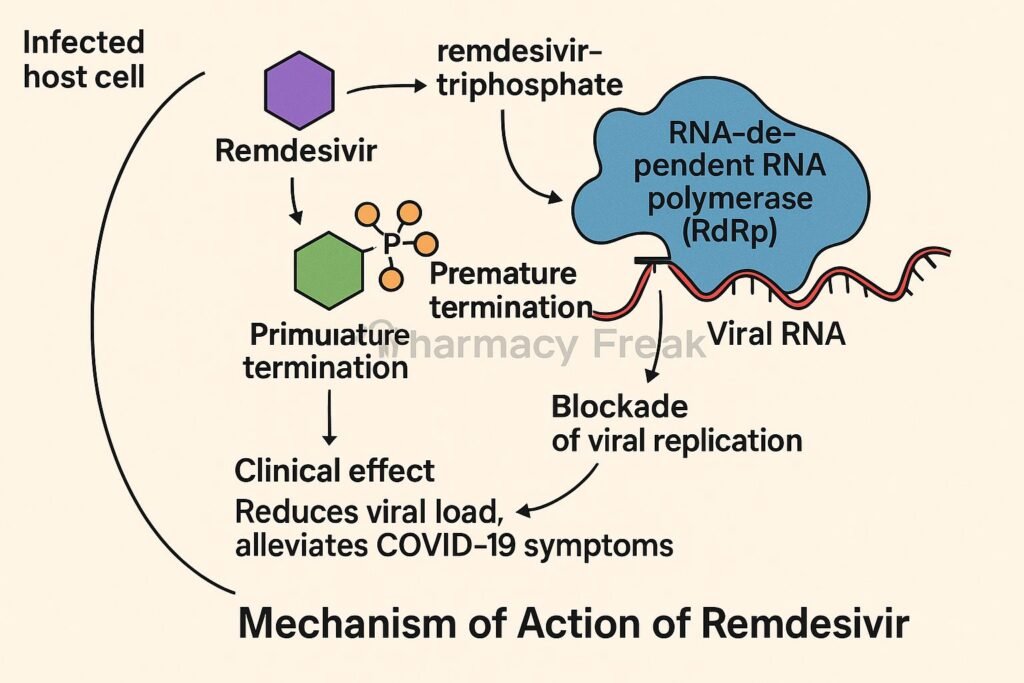
The Mechanism of Action and Patient Selection
Remdesivir functions as a nucleotide analog. By mimicking the building blocks of RNA, it tricks the virus into incorporating the drug into its genetic chain, which subsequently halts the replication process. In the context of the Wuhan coronavirus, this meant that the drug could potentially lower the viral load in the lungs, reducing the severity of the pneumonia associated with SARS-CoV-2.
However, the drug’s administration—requiring intravenous infusion—limited its use to clinical settings. This created a divide between the “hospitalized” patient population and those with mild-to-moderate symptoms who could be treated at home. The trials eventually helped refine the “patient window,” suggesting that the drug is most beneficial for those who are not yet requiring high-flow oxygen or mechanical ventilation, but are showing signs of progression.
The integration of Remdesivir into the broader treatment algorithm often involved combining it with other therapies. The synergy between antivirals (to stop the virus) and anti-inflammatories (to stop the immune system from attacking the lungs) became the gold standard for treating severe COVID-19, significantly lowering the death rate compared to the early days of the pandemic when only supportive care was available.
Challenges in Trial Execution
Conducting phase trials during a global health emergency presented unique hurdles. Researchers faced difficulties in patient recruitment, fluctuating standards of care across different hospitals, and the emergence of new viral variants that could potentially alter the drug’s efficacy. The “noise” in the data from observational studies—where patients were given the drug without a control group—often led to overly optimistic early reports that were later tempered by rigorous randomized trials.
the cost and logistics of delivering intravenous medication globally meant that access was uneven. While high-income countries could implement the drug rapidly, the trials in other regions had to account for varying levels of healthcare infrastructure, which influenced the overall “time to treatment” and, the perceived success of the drug.
What These Trials Mean for Future Pandemics
The legacy of the Remdesivir trials extends beyond a single drug. It established a blueprint for “platform trials,” where multiple treatments can be tested simultaneously against a single control group. This allows researchers to pivot quickly, dropping ineffective treatments and scaling up successful ones without starting new trials from scratch.
The experience also underscored the importance of “adaptive trial design,” where the parameters of a study can be modified based on interim results. This agility was crucial in the fight against the Wuhan coronavirus, allowing the medical community to move from the initial desperation of off-label drug use to a structured, evidence-based therapeutic regimen.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Please consult a licensed healthcare provider for medical diagnosis or treatment options.
As the global health community continues to monitor the evolution of SARS-CoV-2 and other potential zoonotic threats, the data from these phase trials remains a primary reference for antiviral development. The next confirmed checkpoint in this ongoing research involves the monitoring of long-term outcomes for patients treated with antivirals and the evaluation of oral antiviral alternatives that may replace intravenous options in outpatient settings.
We invite you to share your thoughts or questions about the evolution of COVID-19 treatments in the comments below.
Worth a look