
Navigating abdominal surgery in patients with severe cavitary tuberculosis presents a unique set of challenges for anesthesiologists. The delicate lung tissue, already compromised by the infection, is particularly vulnerable to barotrauma – lung injury caused by excessive pressure during mechanical ventilation. A recent case report highlights strategies employed to minimize these risks, offering valuable insights for clinicians managing similar complex cases. The core concern revolves around maintaining adequate oxygenation and ventilation although avoiding further damage to the lungs, a balancing act requiring meticulous planning and execution.
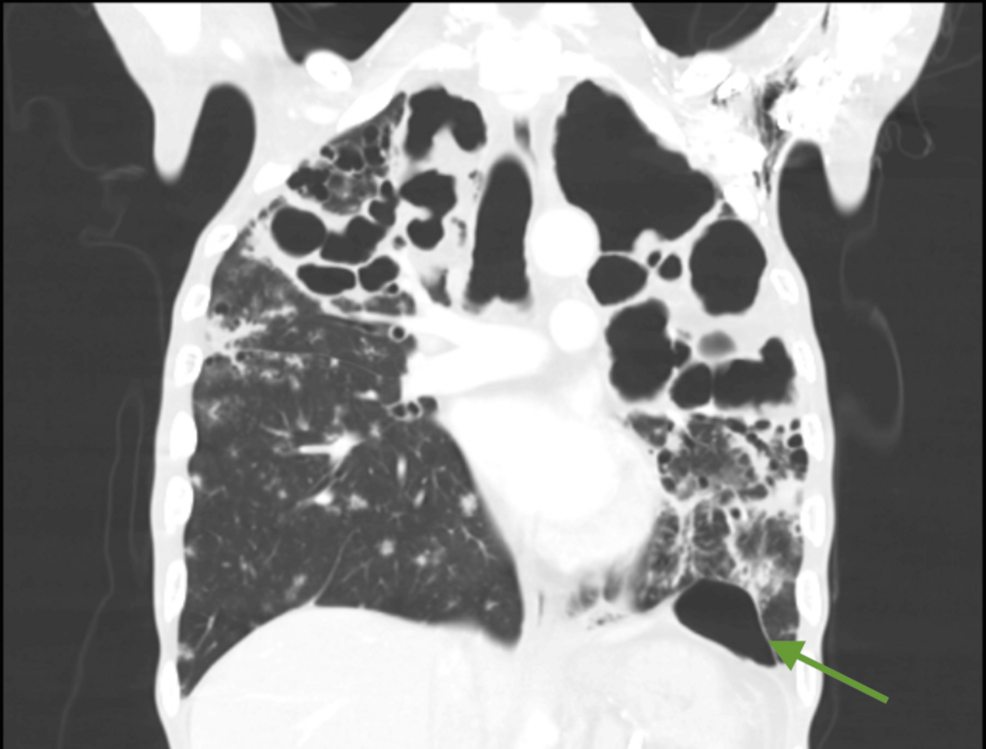
Cavitary tuberculosis, a severe form of the disease, is characterized by the formation of cavities within the lungs. These cavities weaken the lung structure, making it susceptible to rupture during procedures that involve changes in intrathoracic pressure, such as general anesthesia for abdominal surgery. The risk is heightened by the potential for the spread of infection during surgery and the need for prolonged mechanical ventilation postoperatively. Effective anesthetic management, centers on protective lung ventilation strategies and careful monitoring.
Barotrauma can manifest in several ways, including pneumothorax (collapsed lung), pneumomediastinum (air in the space around the heart and lungs), and subcutaneous emphysema (air under the skin). These complications can significantly prolong hospital stays, increase morbidity, and even lead to mortality. Patients with pre-existing lung disease, like severe cavitary tuberculosis, are at a substantially higher risk. According to research published in JAMA Internal Medicine, cardiac involvement is present in 28% to 73% of AIDS patients, highlighting the broader systemic impact of chronic infections and the need for careful cardiovascular monitoring during and after surgery. Cardiac Manifestations of Acquired Immunodeficiency Syndrome
The primary goal during anesthesia is to maintain adequate oxygen levels and carbon dioxide removal while minimizing the pressure applied to the lungs. Here’s achieved through a combination of techniques, including the use of lower tidal volumes (the amount of air delivered with each breath), higher respiratory rates, and positive finish-expiratory pressure (PEEP), which helps to keep the alveoli (tiny air sacs in the lungs) open. Careful selection of neuromuscular blocking agents is also crucial, as these drugs can affect respiratory muscle function.
Strategies for Minimizing Barotrauma: A Case Study Approach
The case report details a patient with severe cavitary tuberculosis undergoing abdominal surgery. The anesthesiology team employed several key strategies to mitigate the risk of barotrauma. First, a thorough pre-operative assessment was conducted to evaluate the patient’s lung function and identify any pre-existing respiratory compromise. This included a review of chest imaging and pulmonary function tests, if available. Second, a lung-protective ventilation strategy was implemented, utilizing low tidal volumes (6 ml/kg of ideal body weight) and moderate PEEP levels.
Continuous monitoring of airway pressures, oxygen saturation, and arterial blood gases was essential throughout the procedure. The team also utilized neuromuscular monitoring to ensure adequate muscle relaxation without compromising respiratory function. Intraoperative fluid management was carefully controlled to prevent overhydration, which can exacerbate lung edema and increase the risk of complications. The use of prone positioning, where the patient is positioned on their stomach, was considered to improve ventilation to the healthier parts of the lung, but was ultimately deemed unsuitable in this particular case due to the nature of the abdominal surgery.
The Role of Anesthetic Agents and Postoperative Care
The choice of anesthetic agents also played a role in minimizing lung injury. Volatile anesthetics, such as sevoflurane and desflurane, were preferred over intravenous anesthetics due to their potential to reduce pulmonary vascular resistance and improve oxygenation. However, the use of these agents requires careful monitoring of the patient’s hemodynamic status.
Postoperatively, continued respiratory support and close monitoring were crucial. The patient was transitioned to non-invasive ventilation as soon as feasible to reduce the need for prolonged intubation. Aggressive pulmonary hygiene, including chest physiotherapy and incentive spirometry, was implemented to prevent atelectasis (lung collapse) and promote lung expansion. Antibiotic therapy was continued to control the tuberculosis infection and prevent secondary bacterial pneumonia.
HIV and Cardiovascular Considerations
It’s important to note the intersection of tuberculosis with other conditions, such as HIV. As highlighted in a 2003 article in Heart, the HIV pandemic has significantly impacted global health, with AIDS becoming a leading cause of death in young adults. HIV AND CARDIOVASCULAR MEDICINE The advent of highly active antiretroviral therapy (HAART) has improved survival rates, but also necessitates consideration of potential cardiac complications. Patients with both tuberculosis and HIV may have a higher risk of cardiovascular dysfunction, requiring careful monitoring of cardiac function during and after surgery.
Managing patients with severe cavitary tuberculosis undergoing abdominal surgery requires a multidisciplinary approach involving anesthesiologists, surgeons, pulmonologists, and infectious disease specialists. By implementing lung-protective ventilation strategies, carefully selecting anesthetic agents, and providing meticulous postoperative care, clinicians can minimize the risk of barotrauma and improve patient outcomes. Further research is needed to refine these strategies and develop new approaches to optimize anesthetic management in this challenging patient population.
The next step in understanding best practices will likely involve larger, multi-center case series and potentially randomized controlled trials to evaluate the efficacy of different ventilation strategies. Continued vigilance and a commitment to individualized patient care remain paramount.
Have you or a loved one faced similar challenges during surgery? Share your experiences and thoughts in the comments below. Please also share this article with anyone who might find this information helpful.